Blepharitis light sensitivity: Causes, Symptoms & Management
How does blepharitis light sensitivity cause light sensitivity? Expert guide covering symptoms, mechanisms, and treatment options.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- Blepharitis causes photophobia primarily through secondary dry eye — MGD (meibomian gland dysfunction) disrupts the tear film lipid layer, destabilizing the tear film and exposing corneal nerve endings.
- Demodex blepharitis (eyelash mite infestation) is more common than previously recognized, particularly in older adults, and requires specific treatment (tea tree oil / terpinen-4-ol lid scrubs).
- Lid hygiene (warm compresses + lid massage + lid scrubs) is the cornerstone of blepharitis treatment and directly reduces photophobia by improving tear film quality.
- Blepharitis is chronic and requires indefinite maintenance treatment — photophobia returns when lid hygiene lapses.
- Omega-3 fatty acid supplementation (EPA/DHA 2–3g/day) improves meibomian gland function and has a meaningful effect on blepharitis-related dry eye and photophobia.
Blepharitis is chronic inflammation of the eyelid margins (the rim of the eyelid where the lashes emerge) and a major contributor to dry eye disease. It is one of the most common causes of eye discomfort worldwide. It produces light sensitivity through a cascade of ocular surface disruption that begins at the lid margin and extends to the cornea.
Why Blepharitis Causes Photophobia

Blepharitis disrupts the tear film and ocular surface through multiple mechanisms that converge to produce photophobia:
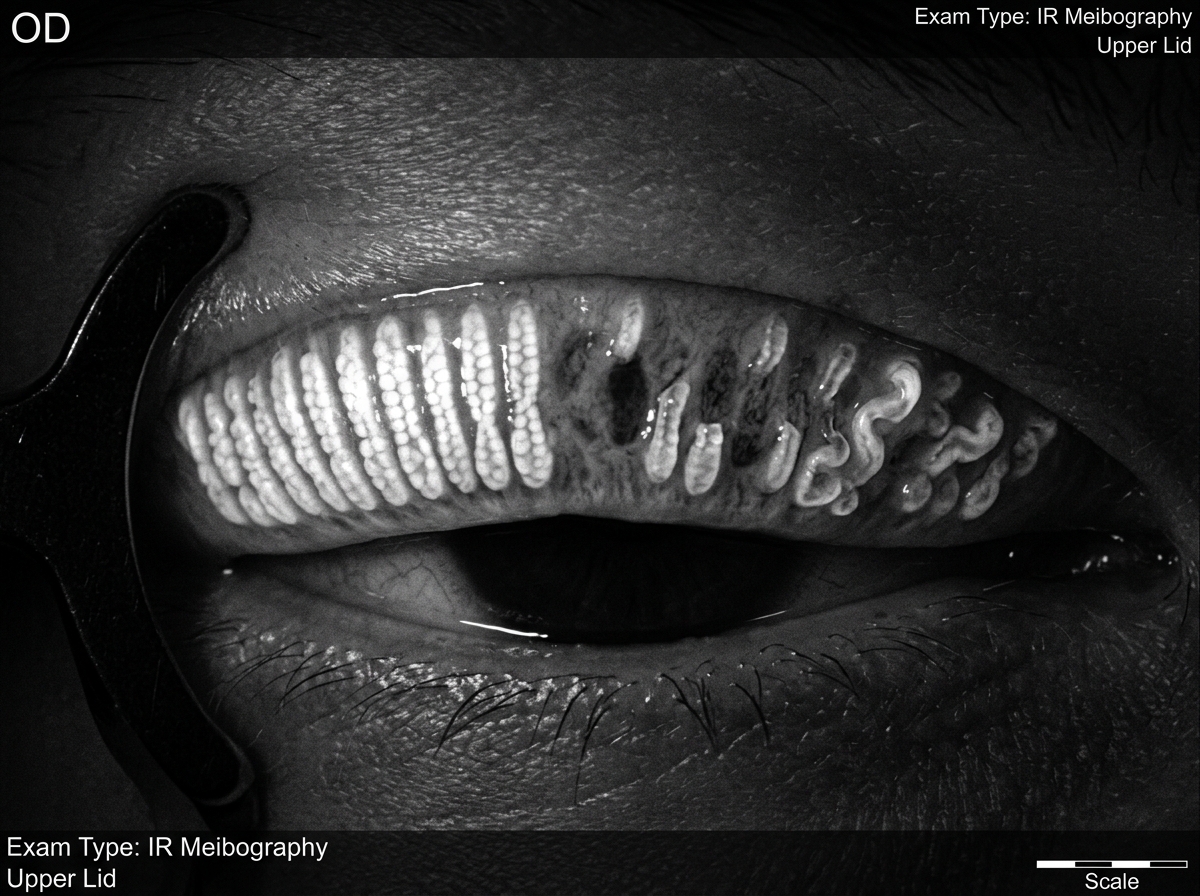
Meibomian gland dysfunction (MGD) . The meibomian glands line the upper and lower eyelid margins and secrete the oily (lipid) layer of the tear film. In posterior blepharitis (the most common type), meibomian glands become obstructed with thickened, waxy secretions. Without the lipid layer, the aqueous tear film evaporates rapidly (evaporative dry eye), exposing corneal nerve endings and triggering photophobia.
Bacterial colonization and toxins. The eyelid margin normally hosts bacteria; in blepharitis, pathological overgrowth of Staphylococcus epidermidis and S. aureus produces exotoxins and lipases that directly damage the tear film and corneal epithelium, sensitizing nerve endings.
Corneal involvement. Chronic blepharitis can cause punctate epithelial erosions, marginal corneal infiltrates, and phlyctenular keratoconjunctivitis — inflammatory lesions driven by hypersensitivity to staphylococcal antigens. These corneal lesions cause intense photophobia and foreign body sensation.
Chronic low-grade inflammation. IL-1, IL-6, MMP-9 and other inflammatory mediators from the inflamed lid margin sensitize corneal and conjunctival nerve fibers, lowering the threshold for light-triggered discomfort.
Types of Blepharitis

Anterior blepharitis — involves the eyelash follicles at the front of the lid margin
- Staphylococcal type: scaly, brittle crusting around lashes; collarettes (sleeve-like crusts around individual lashes); recurrent styes
- Seborrheic type: greasy, soft scales; associated with seborrheic dermatitis of the scalp and face
Posterior blepharitis (meibomian gland dysfunction) — involves the meibomian gland orifices on the inner lid margin; the most common and clinically significant type for photophobia.
Mixed blepharitis — most common; features of both anterior and posterior types.
Diagnosis
Slit-lamp examination reveals:
- Lid margin thickening, telangiectasia, rounding
- Meibomian orifice plugging, toothpaste-like secretions on expression
- Collarettes at lash bases (staphylococcal)
- Conjunctival injection, papillary reaction
- Corneal fluorescein staining (punctate erosions in severe cases)
Treatment
Lid hygiene (cornerstone of treatment):
- Warm compresses 5–10 minutes twice daily — soften meibomian secretions for better expression
- Lid scrubs with diluted baby shampoo or commercial lid wipes (TheraTears SteriLid, OcuSoft) — remove bacterial debris and biofilm
- Meibomian gland expression — manual or device-assisted (LipiFlow, iLux)
Topical treatments:
- Azithromycin ophthalmic solution — anti-inflammatory; reduces MGD
- Topical metronidazole gel — for rosacea-associated blepharitis
- Topical steroids (short-term) — for acute marginal keratitis/phlyctenulosis
Systemic treatments:
- Oral doxycycline 40–100mg daily × 2–3 months — anti-inflammatory (not antibiotic) effect on MGD; reduces MMP-9 and improves meibomian secretion quality; standard of care for rosacea-associated blepharitis
- Omega-3 fatty acids — dietary supplementation reduces meibomian gland inflammation
Photophobia management:
- Treating the underlying blepharitis and MGD resolves the tear film instability that drives photophobia
- Preservative-free artificial tears during treatment to support the disrupted tear film
- Wraparound sunglasses for acute photophobia relief during flares
- FL-41 tinted lenses for fluorescent light sensitivity between flares
Sources
- Lemp MA, Nichols KK. “Blepharitis in the United States 2009.” Ocul Surf. 2009;7(2 Suppl):S1-S14.
- Pflugfelder SC, Karpecki PM, Perez VL. “Treatment of blepharitis: Recent clinical trials.” Ocul Surf. 2014;12(4):273-284.
- Geerling G, et al. “The international workshop on meibomian gland dysfunction.” Invest Ophthalmol Vis Sci. 2011;52(4):1894-2028.