Dry Eye and Light Sensitivity: Why It Happens & How to Treat It
Dry eye syndrome is a leading cause of chronic light sensitivity. Learn the connection between dry eyes and photophobia, and which treatments provide the most relief.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- 1. The Dry Eye–Photophobia Connection
- 2. Understanding Dry Eye Disease: Types and Causes
- 3. The Four Mechanisms Linking Dry Eye to Photophobia
- 4. Recognizing Dry Eye Photophobia: The Characteristic Pattern
- 5. Diagnosing Dry Eye Disease
- 6. Complete Treatment Strategy
- 7. Environmental and Behavioral Management
- 8. Frequently Asked Questions
- 9. Sources
- 40–58% of dry eye disease patients experience photophobia — it's often more disabling than dryness itself.
- Dry eye causes photophobia by exposing corneal nerve endings (the most densely innervated tissue in the body) when the tear film breaks down.
- Lubricating eye drops (artificial tears) and treating the underlying tear film instability can produce rapid, significant photophobia relief.
- Prescription drops (cyclosporine/Restasis, lifitegrast/Xiidra) address the inflammatory component and improve long-term outcomes.
- Screen use, low-humidity environments, contact lens wear, and certain medications all worsen dry-eye photophobia.
The Dry Eye–Photophobia Connection

Dry eye syndrome (DES) is one of the most prevalent and most underappreciated causes of chronic light sensitivity. Studies consistently show that 40–58% of people with dry eye disease experience photophobia as a significant symptom — and for many, the light sensitivity is more disabling day-to-day than the dryness or irritation itself.
The link between dry eye and photophobia is not coincidental. They share overlapping corneal and trigeminal neural pathways that directly amplify each other when both are active. Crucially, the photophobia of dry eye is mechanistically distinct from migraine photophobia — requiring different diagnostic and treatment approaches.
Dry eye disease affects an estimated 344 million people worldwide, making dry eye–related photophobia one of the most common forms of clinically significant light sensitivity globally. Yet it is frequently underrecognized: patients present to physicians for light sensitivity and are not asked about dry eye; or they are treated for dry eye without their photophobia being addressed.
This comprehensive guide covers the complete mechanisms by which dry eye causes photophobia, how to recognize the characteristic symptom pattern, the full spectrum of treatment options, and when specialized care is needed.
Eyes sensitive to light → FL-41 glasses for photophobia → Eye drops for light sensitivity →
Understanding Dry Eye Disease: Types and Causes
What Is Dry Eye Disease?
Dry eye disease (DED) — also called dry eye syndrome (DES) or keratoconjunctivitis sicca (KCS) — is a multifactorial condition of the tear film and ocular surface characterized by symptoms of discomfort, visual disturbance, and tear film instability, potentially causing damage to the ocular surface.
The tear film that coats the cornea and conjunctiva has three layers:
- Lipid layer (outermost): Secreted by meibomian glands ; prevents evaporation
- Aqueous layer (middle): Produced by the lacrimal glands; provides volume
- Mucin layer (innermost): Secreted by goblet cells; anchors the tear film to the ocular surface
Disruption of any layer produces dry eye disease.
Types of Dry Eye Disease

Evaporative dry eye (most common, ~86% of cases): The tear film evaporates too rapidly. Most commonly caused by meibomian gland dysfunction (MGD) — obstruction or dropout of the oil-secreting meibomian glands in the eyelid margins. Other evaporative causes: incomplete blink (screen users), low blink rate, lid abnormalities, contact lens wear.
Aqueous-deficient dry eye: Insufficient tear volume produced. Major causes:
- Sjögren’s syndrome (primary and secondary) — autoimmune destruction of lacrimal glands; produces severe aqueous-deficient dry eye
- Non-Sjögren’s aqueous-deficient DED: Lacrimal gland damage from radiation, sarcoidosis, graft-versus-host disease, medication effects (antihistamines, antidepressants, diuretics)
Mixed type: Most patients have elements of both evaporative and aqueous-deficient dry eye; the distinction is more conceptual than strictly clinical.
Risk Factors for Dry Eye Disease
| Category | Specific Factors |
|---|---|
| Demographic | Female sex, age > 50, Asian ethnicity |
| Environmental | Low humidity, high wind, air conditioning, high altitude |
| Behavioral | Extended screen use, contact lens wear, LASIK |
| Medical | Sjögren’s, rheumatoid arthritis, thyroid disease, rosacea, blepharitis, diabetes |
| Medications | Antihistamines, antidepressants, antipsychotics, diuretics, isotretinoin, beta-blockers |
| Nutritional | Omega-3 deficiency, vitamin A deficiency |
The Four Mechanisms Linking Dry Eye to Photophobia
Mechanism 1: Corneal Nerve Sensitization (The Primary Mechanism)
The cornea is the most densely innervated tissue in the human body — containing approximately 7,000 nerve endings per square millimeter, compared to 200/mm² in skin. This extreme innervation is why corneal pathology produces such severe symptoms.
In dry eye disease, the corneal surface becomes unstable. Tear film breakup exposes the corneal epithelium to the environment, creating localized desiccation stress that chronically activates the dense network of polymodal nociceptors — sensory nerves that respond to dryness, temperature, chemical irritants, and mechanical stimuli.
With persistent activation, these corneal nerves undergo peripheral sensitization: their firing threshold decreases, their spontaneous activity increases, and they begin firing in response to stimuli that would normally be subthreshold — including light. This is the primary mechanism of dry eye–associated photophobia.
The nerve signals travel via the nasociliary branch of the ophthalmic division of the trigeminal nerve to the trigeminal nucleus caudalis in the brainstem, then ascend to the thalamus and somatosensory cortex, where they are interpreted as eye pain and photophobia.
Mechanism 2: Central Sensitization
With prolonged peripheral sensitization, the central nervous system undergoes central sensitization — a state where dorsal horn and trigeminal nucleus neurons become hyper-responsive, amplifying all incoming signals.
In chronic dry eye, central sensitization means:
- Normal light exposure generates disproportionately large pain responses
- Photophobia persists even when the corneal surface is temporarily lubricated (because the central amplification is now autonomous)
- Patients may develop photophobia even with eyes closed (since even eyelid skin transmits some light to photoreceptors)
- The condition becomes difficult to treat with eye drops alone — central sensitization requires central-acting treatments
This is the mechanism underlying neuropathic ocular pain — a recognized complication of severe chronic dry eye where pain persists beyond what corneal surface findings would predict. Neuropathic dry eye pain is notoriously difficult to treat.
Mechanism 3: Disrupted Tear Film Optics
A healthy, stable tear film provides a smooth, continuous optical surface across the cornea. When the tear film breaks up (as in dry eye), it creates:
- Irregular light refraction — instead of uniform refraction, different areas of the cornea refract light at different angles
- Increased light scatter — irregular surface creates diffuse scatter that reduces image quality
- Glare sensitivity — particularly to bright or point sources of light
The visual consequence: the brain receives degraded, scattered visual input, requiring increased neural processing effort to extract a clear image. This increased processing demand at normal light levels manifests as visual discomfort, fatigue, and light sensitivity — even before pain is involved.
The 20-20-20 correlation: Blink rate decreases by 60–70% during screen use (from ~15 blinks/minute to ~5/minute). Each blink re-spreads the tear film; reduced blinking accelerates tear film breakup. This explains why screen time dramatically worsens photophobia in dry eye patients.
Mechanism 4: Inflammatory Amplification
Dry eye disease involves a self-perpetuating cycle of ocular surface inflammation:
- Tear film instability → hyperosmolar tears
- Hyperosmolar tears → activation of inflammatory signaling (MAPK, NF-κB pathways)
- Inflammatory cytokines (IL-1, TNF-α, MMP-9) released by corneal epithelial cells
- Cytokines activate immune cells (dendritic cells, T lymphocytes) in the ocular surface
- Activated immune cells release further inflammatory mediators
- Inflammatory mediators sensitize corneal nociceptors
- Return to step 1 (perpetuating cycle)
This inflammatory cycle directly amplifies corneal nerve sensitization and photophobia. Breaking the inflammatory cycle — not just lubricating the surface — is essential for sustained photophobia relief.
Recognizing Dry Eye Photophobia: The Characteristic Pattern
Dry eye photophobia has a distinctive symptom profile that distinguishes it from migraine or post-concussion photophobia:
The Telltale Features
| Feature | Dry Eye Photophobia | Migraine Photophobia |
|---|---|---|
| Time of day | Worsens through the day | Can be any time; often morning on waking |
| Triggers | Screen use, air conditioning, wind, dry environments | Bright light, flickering, glare |
| Associated symptoms | Burning, stinging, foreign body sensation, blurred vision | Headache, nausea, phonophobia |
| Blinking effect | Blinking temporarily improves vision and comfort | No effect |
| Artificial tears effect | Provides temporary improvement | Little/no effect |
| Fluorescent light | Particularly problematic | Also problematic |
| Eye appearance | May be red, watery, or visibly dry | Often normal |
The Diurnal Pattern
Dry eye photophobia characteristically worsens throughout the day. The tear film is relatively stable in the morning and deteriorates progressively with prolonged use and environmental exposure. Many dry eye patients report that their worst photophobia is in the late afternoon and evening, after hours of screen use.
This contrasts with migraine photophobia, which tends to be episodic and unpredictable in timing, or post-concussion photophobia, which may be relatively constant.
Diagnosing Dry Eye Disease
Dry eye diagnosis is made by an ophthalmologist or optometrist and typically involves:
Symptom questionnaires: The Ocular Surface Disease Index (OSDI) is the most widely used validated questionnaire; scores ≥13 indicate at least mild dry eye; ≥33 indicates moderate-severe.
Tear film assessment:
- Tear breakup time (TBUT): Fluorescein dye instilled; time until tear film shows first break under slit lamp with blue light. TBUT < 10 seconds = abnormal; < 5 seconds = severe
- Schirmer’s test: Strips of paper placed in lower lid; measure tear production volume; < 5mm/5min = aqueous-deficient dry eye
Ocular surface staining:
- Fluorescein staining: reveals corneal epithelial damage
- Lissamine green or rose bengal staining: reveals conjunctival epithelial damage
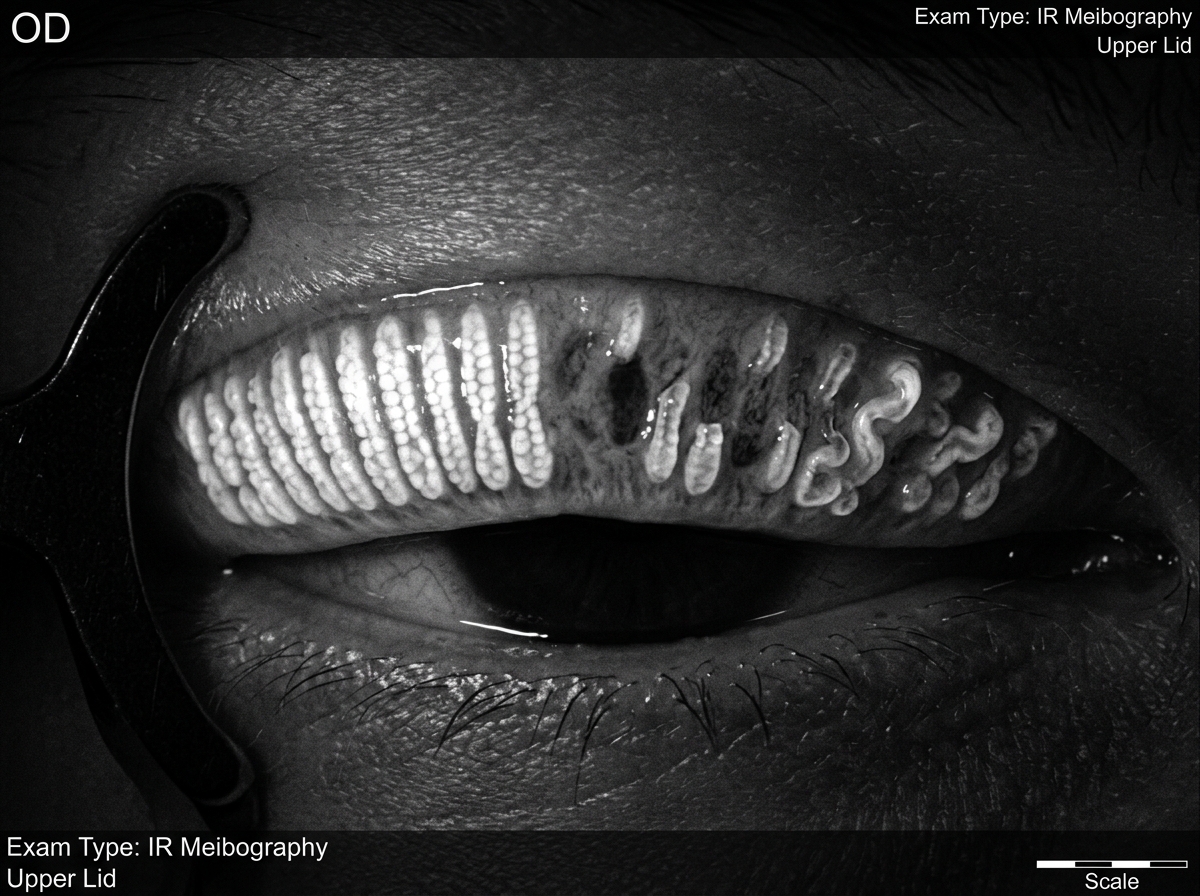
Meibomian gland evaluation:
- Meibography: infrared imaging of meibomian glands; reveals gland dropout and morphology
- Meibomian gland expression: assessment of secretion quality and quantity
Inflammatory markers:
- InflammaDry (MMP-9 test): rapid in-office point-of-care test; elevated MMP-9 in tears indicates ocular surface inflammation
Complete Treatment Strategy
Step 1: Artificial Tears (All Dry Eye Patients)
Preservative-free formulations are essential for frequent use. Preservatives — especially benzalkonium chloride (BAK) — are toxic to corneal epithelial cells and worsen dry eye with frequent use.
Recommended formulations by tear film deficiency:
For aqueous-deficient dry eye:
- Carboxymethylcellulose (CMC): Refresh Tears, Optive
- Sodium hyaluronate (hyaluronic acid): Hylo, Blink Tears
- Polyethylene glycol/propylene glycol: Systane Ultra
For evaporative dry eye (lipid layer deficiency):
- Lipid-containing drops: Systane Complete, Refresh Optive Advanced, Soothe XP
- These restore the lipid layer and extend tear film stability
Frequency: Use as often as needed for comfort — preservative-free drops can be used every 30–60 minutes if necessary. For photophobia management, using drops before engaging in visually demanding tasks (screen work, driving) can reduce peak photophobia severity.
Step 2: Prescription Treatments (Moderate-Severe Dry Eye)
Cyclosporine A 0.05% (Restasis): Immunosuppressant that reduces T-cell–mediated lacrimal gland inflammation, improving tear production over time. Onset of benefit: 3–6 months of twice-daily use. Effective for Sjögren’s and non-Sjögren’s aqueous-deficient dry eye.
Lifitegrast 5% (Xiidra): LFA-1 integrin antagonist that blocks T-cell adhesion and corneal inflammation. Faster onset than cyclosporine (some benefit at 2 weeks; significant improvement at 3 months). The only prescription dry eye medication specifically trialed for photophobia as a secondary endpoint — demonstrating significant photophobia reduction.
Cyclosporine 0.09% (Cequa): Nanomicellar formulation of higher-concentration cyclosporine; may be more effective than 0.05% in severe cases.
Varenicline nasal spray (Tyrvaya): Stimulates trigeminal parasympathetic reflex, increasing tear secretion. Novel delivery route useful for patients who cannot tolerate eye drops.
Autologous serum eye drops: Blood is drawn from the patient; serum is separated and diluted; the resulting drops contain growth factors, vitamins, and proteins matching natural tears. Highly effective for severe or neuropathic dry eye; requires compounding pharmacy preparation.
Step 3: Meibomian Gland Treatment (Evaporative Dry Eye)
Warm compresses: Apply warm, moist heat to closed eyelids for 10–15 minutes daily. Liquefies meibomian secretions, allowing better expression. Effective but requires consistent daily practice.
Eyelid hygiene/scrubs: Removes bacterial biofilm from lid margins (which degrades meibomian secretions). Foam cleansers (Ocusoft), hypochlorous acid sprays (Avenova), or commercially available lid scrub pads.
Omega-3 fatty acid supplementation: Improves meibomian gland secretion quality. Use re-esterified triglyceride (rTG) form for best bioavailability. Dose: 1,000–2,000 mg EPA+DHA daily. Give 3–6 months for full effect.
Thermal pulsation (LipiFlow): FDA-cleared in-office device that simultaneously applies controlled heat (42.5°C) to the inner eyelid and pulsatile pressure to the outer lid, liquefying and expressing meibomian gland contents. Most effective single in-office treatment for MGD. Effect lasts 9–12+ months. Cost: $600–1000 (typically not insurance covered).
Intense Pulsed Light (IPL): Originally a skin rejuvenation technology; applied to periocular skin, IPL treats rosacea-associated meibomian gland dysfunction, reduces Demodex mite burden, and improves meibomian gland function. Emerging as an effective option for evaporative dry eye with rosacea component. Requires a series of 3–4 treatments.
Step 4: Photophobia-Specific Interventions
FL-41 tinted lenses: Filter the 450–530 nm blue-green wavelength band most activating for the photophobia pain pathway. Significantly reduce photophobia without causing dark adaptation. Appropriate for indoor wear. The most evidence-based eyewear for dry eye–associated photophobia. FL-41 glasses guide →
Scleral contact lenses: Semi-rigid lenses that vault over the cornea, resting on the sclera, filled with a fluid reservoir (saline) that maintains constant hydration of the corneal surface. For severe dry eye photophobia (particularly post-refractive surgery, Sjögren’s, graft-vs-host disease), sclerals can dramatically reduce photophobia by maintaining the corneal nerve environment in a stable, moist state. Require fitting by a specialized contact lens practitioner.
Moisture chamber spectacles: Wraparound frames with sealed side panels that create a humid microenvironment around the eyes, reducing evaporation. Available as standalone eyewear (Wiley X, 7eye) or as inserts that fit over existing glasses. Particularly valuable in windy, air-conditioned, or low-humidity environments.
Step 5: Addressing Neuropathic Ocular Pain
For patients with chronic, severe dry eye photophobia that persists despite adequate treatment of the ocular surface, neuropathic pain mechanisms may be driving symptoms:
Low-dose naltrexone (LDN): 1.5–4.5 mg nightly; modulates opioid receptors and reduces neuroinflammation; emerging evidence for neuropathic ocular pain Low-dose amitriptyline: Tricyclic antidepressant at sub-antidepressant doses (10–25 mg) modulates trigeminal pain processing Oral gabapentin/pregabalin: May reduce neuropathic corneal pain; used off-label Compounded topical agents: Autologous serum, neurotrophic eye drops (cenegermin/Oxervate) for corneal nerve regeneration
Environmental and Behavioral Management
Creating a Dry-Eye-Friendly Home Environment
- Humidifier: Maintain indoor humidity at 40–60%; dry eye worsens in humidity < 30%
- Air filtration: HEPA filters reduce airborne irritants that exacerbate dry eye symptoms
- Air circulation: Avoid air vents, fans, or air conditioning directed at the face
- Lighting: Warm-white LED (2700–3000K) reduces the blue-heavy spectrum that worsens photophobia; minimize fluorescent lights
Screen Hygiene
- Apply the 20-20-20 rule consistently: every 20 minutes, look 20 feet away for 20 seconds (allows tear film recovery)
- Artificial tear instillation before screen sessions reduces cumulative desiccation
- Screen brightness reduction — screen should not be brighter than the room ambient light
- Matte anti-glare screen protectors reduce reflective glare that worsens photophobia
- Consider blue-light-filtering screen protectors for screen-heavy work environments
Blink Training
Consciously practice complete, full blinks (where upper lid reaches lower lid) while working at screens. Most screen-induced blinks are incomplete, providing inadequate tear film resurfacing.
Frequently Asked Questions
Can dry eye cause permanent photophobia? Most dry eye–associated photophobia is reversible with effective treatment of the underlying condition. However, if neuropathic changes develop from chronic untreated severe dry eye (particularly post-refractive surgery or severe Sjögren’s), photophobia may persist even after the ocular surface is improved. Early treatment prevents progression to neuropathic pain.
Does crying make dry eye worse? Emotional tears are different from the basal tears maintained by the lacrimal glands — they are produced rapidly and are less well-balanced in electrolytes. Prolonged crying can temporarily worsen dry eye symptoms, though the excess tear production during crying provides temporary surface hydration.
Is LASIK a risk factor for dry eye photophobia? Yes — LASIK corneal flap creation severs corneal nerves, causing post-LASIK dry eye syndrome in 30–50% of patients in the first 6–12 months. Corneal nerve regeneration typically restores sensation and dry eye resolves over 12 months, but some patients develop persistent post-LASIK dry eye and photophobia. LASIK candidates should be counseled about this risk.
Can contact lens wear cause photophobia? Yes — contact lens wear is a significant risk factor for dry eye and dry eye–associated photophobia. Contact lenses disrupt the lipid layer of the tear film and can cause hypoxic and desiccation stress on the cornea. Switching to higher-oxygen-permeability lenses, using lubricating drops, or switching to glasses can reduce symptoms.
Sources
- Galor A, et al. “Neuropathic ocular pain: an important yet underevaluated feature of dry eye.” Eye. 2018;32(5):820-821.
- Crane AM, et al. “Prevalence of photosensitivity in dry eye disease.” Cornea. 2021.
- Goyal S, Hamrah P. “Understanding Neuropathic Corneal Pain.” Seminars in Ophthalmology. 2016;31(1-2):59-70.
- Belmonte C, et al. “TFOS DEWS II pain and sensation report.” Ocular Surface. 2017;15(3):404-437.
- Craig JP, et al. “TFOS DEWS II Report Executive Summary.” Ocular Surface. 2017;15(4):802-812.
- Baudouin C, et al. “Role of hyperosmolarity in the pathogenesis and management of dry eye disease.” Ocular Surface. 2013;11(4):246-258.
- Galor A, et al. “Persistent Dry Eye Symptoms After Topical Cyclosporine Treatment.” JAMA Ophthalmology. 2019.