FL-41 Glasses: The Clinically Proven Lens for Photophobia & Migraine
FL-41 tinted glasses are the most clinically studied eyewear for photophobia and migraine. Learn how they work, what the research shows, and how to choose the right pair.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- 1. What Are FL-41 Glasses?
- 2. The Science: Why Specific Wavelengths Matter
- 3. The Complete Clinical Evidence Base
- 4. How FL-41 Compares to Every Alternative
- 5. Who Should Use FL-41 Glasses: By Condition
- 6. The Critical Warning: Avoiding Dark Adaptation
- 7. Choosing FL-41 Glasses: Complete Buying Guide
- 8. How to Use FL-41 Glasses Effectively
- 9. When FL-41 Is Not Enough
- 10. Frequently Asked Questions
- 11. Sources
- FL-41 is the most clinically studied tinted lens for photophobia — multiple randomized trials show significant reduction in migraine frequency and light sensitivity.
- The FL-41 tint blocks wavelengths in the 480–500 nm range, which are the most activating for sensitized thalamic pain pathways.
- FL-41 lenses are light enough for comfortable all-day indoor wear, unlike dark sunglasses that worsen dark adaptation.
- Available as prescription or non-prescription; TheraSpecs and Axon Optics are the most clinically-tested brands.
- Effect is typically noticeable within 1–2 weeks of consistent use; full assessment should be made after 4–6 weeks.
What Are FL-41 Glasses?

FL-41 is a rose-pink tinted lens that selectively filters a specific band of visible light wavelengths — primarily the 450–530 nm blue-green range — that research has identified as the most activating for the photophobia pain pathway. Originally developed in Birmingham, UK in the early 1990s to reduce discomfort from fluorescent lighting, FL-41 has since become the most clinically studied eyewear intervention for chronic photophobia, migraine, and post-concussion light sensitivity.
Unlike dark sunglasses (which block light broadly and cause dark adaptation) or standard blue-light-blocking glasses (which filter a different, shorter wavelength range), FL-41 is specifically calibrated for the neurological photophobia mechanism — filtering the wavelengths that most powerfully activate the retino-thalamic pain pathway while transmitting enough light for comfortable indoor use without dark adaptation.
This comprehensive guide covers the neuroscience behind FL-41, the complete clinical research evidence, how to choose lenses, how to use them correctly, and how they compare to every alternative.
Blue light glasses → All photophobia treatments → Photophobia guide →
The Science: Why Specific Wavelengths Matter
The Photophobia Pain Pathway
Photophobia is not simply “eyes being sensitive to brightness” — it is a specific pain pathway activated by light. Understanding this pathway is essential to understanding why FL-41 works.
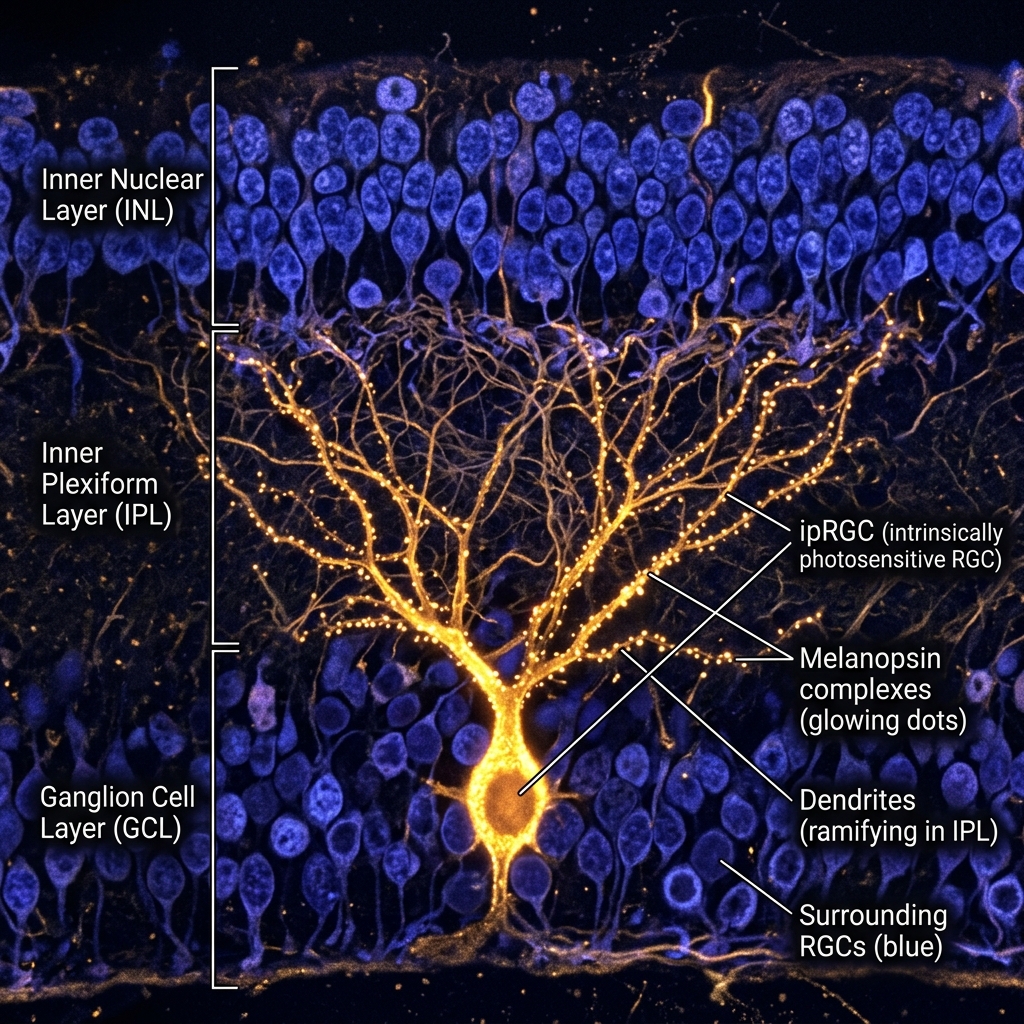
The retina contains intrinsically photosensitive retinal ganglion cells (ipRGCs) — a small population of ganglion cells (~2% of total) containing the photopigment melanopsin. These cells do not form images; they detect ambient light intensity and drive:
- The pupillary light reflex
- Circadian rhythm synchronization
- The photophobia pain pathway via direct projections to the posterior thalamus
The ipRGCs have peak melanopsin sensitivity at approximately 480 nm — squarely in the blue-green range. When the thalamus is sensitized (as in migraine, concussion, or chronic photophobia), ipRGC signals from blue-green light produce disproportionate pain responses.
The wavelength research: Studies by Noseda and Burstein (Harvard, 2010–2016) directly measured the electrical signals generated in the photophobia pain pathway by different wavelengths. Blue and blue-green light (450–530 nm) produced the strongest thalamic pain responses. Green light at ~520 nm produced the weakest responses. Red light was intermediate.
Why FL-41’s Wavelength Band Was Chosen
FL-41 filters the 450–530 nm range — exactly the band identified as most activating for the photophobia pain pathway. The tint was originally empirically developed (before the ipRGC research) by researchers at the University of Birmingham observing that rose-pink tinted lenses reduced migraine frequency in photophobic children. The neuroscience subsequently explained the mechanism.
The rose-pink appearance of FL-41 results from filtering the blue-green channel while transmitting red and some yellow wavelengths — creating the characteristic warm, pink-tinted visual appearance.
The Complete Clinical Evidence Base
Pediatric Migraine and Photophobia (1991)

The landmark study by Good et al. (1991) in Developmental Medicine and Child Neurology examined children aged 7–16 with migraine and photophobia. Children wearing FL-41 tinted lenses experienced a significant reduction in migraine attack frequency compared to children wearing control (non-therapeutic pink) tinted lenses. This was a blinded, controlled trial — the control lens appeared similar but did not filter the therapeutic wavelength range.
Key finding: FL-41 specifically (not just any pink tint) reduced migraine frequency, establishing that the wavelength selectivity — not placebo or comfort — drove the benefit.
Blepharospasm Studies
Blepharospasm (benign essential blepharospasm, BEB) is a neurological condition causing involuntary, forceful eye closure — and is perhaps the most extreme form of photophobia-driven disability. Patients with blepharospasm often cannot keep their eyes open in normal lighting.
Blackburn et al. (1991) in Ophthalmology found FL-41 tinted lenses significantly improved blepharospasm symptoms — reducing both the frequency and force of involuntary spasm episodes. This blepharospasm evidence is the strongest single-condition evidence base for FL-41, representing a condition with highly objective outcomes (spasm frequency can be measured and filmed).
Subsequent studies consistently replicated these findings across multiple research groups.
Migraine Photophobia in Adults (2010)
Katz and Digre at the University of Utah’s Moran Eye Center — the leading U.S. center for photophobia research — conducted controlled studies demonstrating that FL-41 tinted spectacles significantly reduced interictal photophobia (light sensitivity between migraine attacks) in adult migraineurs. Patients reported improved light tolerance and reduced headache frequency with consistent FL-41 wear.
Post-Concussion and TBI Research
Post-concussion photophobia is one of the most common and debilitating post-concussion symptoms, affecting 50–80% of concussion patients at some stage of recovery. The University of Utah’s research group found FL-41 tinted lenses significantly reduced photophobia in patients with post-concussion syndrome and traumatic brain injury, improving both subjective comfort and functional light tolerance.
This evidence is particularly important because post-concussion photophobia is often persistent and refractory — FL-41 provides meaningful relief even in cases where the photophobia has not resolved with time alone.
Post-concussion photophobia guide →
Retrospective and Real-World Data
TheraSpecs — the most widely available FL-41 brand, developed in collaboration with the University of Utah — has compiled retrospective outcome data from thousands of users:
- 86% reported reduced light sensitivity
- 74% reported reduced migraine frequency with consistent wear
- 68% reported improved screen tolerance
- 82% reported improved function in fluorescent-lit environments
While retrospective data cannot establish causation with the same rigor as blinded trials, these real-world numbers across a large population consistently support the clinical trial findings.
How FL-41 Compares to Every Alternative
FL-41 vs. Blue Light Glasses
| Feature | FL-41 | Blue Light Glasses |
|---|---|---|
| Primary filter band | 450–530 nm (blue-green) | 380–450 nm (violet-blue) |
| Target mechanism | Migraine photophobia pain pathway | Screen-related eye strain, sleep |
| Clinical evidence | Multiple RCTs in migraine, TBI | Limited for eye strain; some for sleep |
| Photophobia use | ✅ Specifically indicated | ⚠️ Partial overlap only |
| Dark adaptation risk | No (light enough for indoor wear) | No |
| Indoor use | ✅ Primary use | ✅ |
| Cost | $80–200+ | $20–100 |
Bottom line: Standard blue light glasses filter a different wavelength range (violet-blue, 380–450 nm) than FL-41 (450–530 nm, blue-green). They address a different mechanism. For migraine and neurological photophobia, FL-41 is more directly targeted. For evening screen use to improve sleep, amber blue-light-blocking glasses are preferred.
FL-41 vs. Dark Sunglasses (Indoors)
This comparison reflects one of the most important safety considerations in photophobia management:
Dark sunglasses indoors cause dark adaptation — the visual system recalibrates to low-light conditions, making normal light increasingly painful when the glasses are removed. This creates a dependency cycle that progressively worsens photophobia over months to years.
FL-41 lenses, with approximately 35–40% visible light transmission, are specifically designed to be light enough to prevent dark adaptation while still providing meaningful spectral filtering. They are the appropriate eyewear for indoor use by photophobic individuals — not dark sunglasses.
The only appropriate indoor use of dark lenses is during a severe acute migraine attack — as a temporary relief measure — not as everyday management.
FL-41 vs. Photochromic (Transition) Lenses
Photochromic lenses darken outdoors in UV light and lighten indoors. The problem for photophobia: outdoors, they become very dark (causing dark adaptation if worn regularly), and they don’t reach full darkness in cars (windshields block the UV that activates them). Indoors, they are essentially clear — providing no spectral filtering.
FL-41 provides consistent filtering indoors regardless of UV conditions. The two can be combined: prescription FL-41 lenses with photochromic darkening allow one pair to serve both indoor and outdoor purposes — though for severe photophobia, separate indoor FL-41 and outdoor polarized sunglasses are preferred.
FL-41 vs. Polarized Sunglasses
Polarized lenses reduce glare from horizontal reflective surfaces (water, roads, snow). They do not selectively filter the photophobia-activating wavelength band. Excellent for outdoor use — not a substitute for FL-41 for indoor or neurological photophobia.
For outdoor use, FL-41 with added polarization (available from some specialty brands) provides both benefits.
Who Should Use FL-41 Glasses: By Condition
Migraine (All Types)
FL-41 is indicated for:
- Interictal photophobia (between attacks) — the most common daily disability from migraine; FL-41 significantly reduces functional impairment
- Ictal photophobia (during attacks) — used in combination with dark environment rest during attacks
- Chronic migraine — daily FL-41 wear as part of a comprehensive management plan alongside preventive medications
Migraine and light sensitivity →
Post-Concussion Syndrome
FL-41 is a first-line recommendation from most concussion rehabilitation specialists for post-concussion photophobia. Key considerations:
- Use FL-41 rather than dark sunglasses — dark lenses worsen long-term photophobia
- Begin wear as soon as post-concussion photophobia becomes functionally limiting
- Combine with graded exposure to light as part of the rehabilitation plan
- Most post-concussion photophobia improves substantially over 3–12 months; FL-41 supports function during this recovery period
Post-concussion light sensitivity →
Blepharospasm
The strongest single evidence base for FL-41. Patients with blepharospasm often experience dramatic improvement with consistent FL-41 wear. Botulinum toxin (Botox) injections remain the primary treatment, but FL-41 serves as an important adjunct.
Dry Eye Disease
FL-41 is not a treatment for dry eye itself, but photophobia from dry eye — which is driven by corneal nerve sensitization — is often significantly reduced by FL-41 filtering of the triggering wavelength band. Used in combination with artificial tears and dry eye treatment.
Dry eye and light sensitivity →
Autism Spectrum Disorder
Sensory hypersensitivity including photophobia is extremely common in autism. FL-41 lenses are widely used by autistic individuals with photophobia, reducing the sensory overload from fluorescent lighting in school and work environments. Anecdotal and retrospective data is positive; formal clinical trials in autism specifically are limited.
General Photophobia of Any Cause
For any photophobic individual who has not yet found relief, FL-41 is the appropriate first-line eyewear trial — whether the cause is migraine, dry eye, post-concussion, medication effects, lupus, MS, or idiopathic photophobia.
The Critical Warning: Avoiding Dark Adaptation
This is the most clinically important point in photophobia management and the most frequently violated by patients:
Never wear dark sunglasses indoors as a photophobia management strategy.
Dark sunglasses indoors trigger the following cascade:
- Reduced retinal illumination → pupil dilation
- Retinal dark adaptation → increased photoreceptor sensitivity
- Removal of dark glasses → normal light seems extremely bright/painful
- Patient increases dependence on dark glasses
- Visual system progressively dark-adapts further
- Normal ambient lighting becomes progressively more painful
This is not theoretical — multiple specialist clinics report patients who have been wearing dark sunglasses indoors for months or years and whose photophobia has dramatically worsened as a result.
FL-41 lenses are the solution: they filter the specific triggering wavelength band without causing dark adaptation. This is why their ~35–40% light transmission is not a design limitation — it is a carefully chosen protective feature.
Choosing FL-41 Glasses: Complete Buying Guide
Tint Density and Transmission
Authentic FL-41 lenses should transmit approximately 35–40% of visible light (medium density). This transmission level:
- Provides meaningful filtering of the 450–530 nm band
- Avoids dark adaptation
- Allows comfortable indoor use without significant vision impairment
Red flags to avoid:
- Very dark “FL-41” lenses (< 20% transmission) — cause dark adaptation
- Very pale/clear “FL-41” lenses (> 60% transmission) — insufficient filtering
- Generic “rose tint” lenses without FL-41 wavelength specification — may not target the correct band
Prescription vs. Non-Prescription
Prescription FL-41 is strongly preferred for regular wear. Wearing incorrectly powered lenses for extended periods causes accommodative strain that worsens headache and eye discomfort. If you wear glasses or contact lenses, have FL-41 prescription lenses made.
Non-prescription FL-41 (plano lenses) is appropriate for:
- Contact lens wearers who want an overlay option
- Users with no refractive error
- Initial trial before committing to prescription lenses
Frame Style and Coverage
Wraparound frames: Provide the most complete protection from peripheral light — important for individuals with severe photophobia or blepharospasm who are sensitive to light entering from the sides.
Oversized frames: Provide more coverage without the sporty appearance of wraparounds — suitable for work environments where professional appearance matters.
Standard frames: Appropriate for mild-moderate photophobia where peripheral light is not a primary concern.
Lens Material
- Polycarbonate — Most impact resistant; standard recommendation for children and active use; some minor optical distortion at edges
- CR-39 plastic — Good optical clarity; lighter than glass; standard for adult everyday lenses
- High-index plastic — Required for high prescriptions to avoid thick lenses; excellent optics
- Glass — Best optical clarity; significantly heavier; not recommended for children or sport use
Top Brands
TheraSpecs — The leading clinical FL-41 brand; developed in collaboration with the University of Utah’s photophobia research program; available in prescription and non-prescription; multiple frame styles from discrete wraparounds to standard frames; the brand used in most U.S. photophobia clinical studies.
Axon Optics — Another medically-focused FL-41 brand with evidence-based tint formulation; prescription and non-prescription; comparable to TheraSpecs in quality.
Optical labs/custom lenses — Many optical labs can apply FL-41 tint to custom prescription lenses; specify “FL-41 tint at 35–40% transmission” or show the lab TheraSpecs or Axon Optics tint specifications for matching.
How to Use FL-41 Glasses Effectively
Consistent Daily Wear
Clinical studies consistently show that FL-41 benefit builds over time with consistent wear, rather than providing immediate dramatic relief. Most patients report:
- Some improvement within the first 1–2 weeks
- Meaningful improvement by 4–6 weeks
- Maximum benefit by 8–12 weeks of consistent daily wear
This time-course is consistent with the gradual normalization of thalamic sensitivity through reduced daily photophobia stimulation.
Practical guidance: Wear FL-41 whenever in challenging lighting conditions — indoors with fluorescent or cool-white LED lighting, at the computer, in grocery stores and offices. Do not limit wear to “bad days” — consistent preventive use is more effective than reactive use.
Combining FL-41 with Other Treatments
FL-41 is most effective as part of a comprehensive photophobia management plan:
- Treat the underlying condition — FL-41 manages symptoms but does not treat migraine, dry eye, or other causes. Pursue definitive treatment alongside FL-41 wear.
- Environmental modifications — Replace home lighting with warm-white LED (2700–3000K); use dimmer switches; reduce screen brightness. FL-41 and environmental modifications are complementary, not alternatives.
- Graded light exposure — Under specialist guidance, gradually increase exposure to normal lighting conditions to prevent progressive dark adaptation.
- Preserve sunglasses for outdoors — Use polarized sunglasses outdoors; switch to FL-41 indoors. Do not use sunglasses as the indoor eyewear.
Tracking Progress
Keep a photophobia and headache diary before starting FL-41 and for the first 8–12 weeks of use. Record:
- Daily photophobia severity (0–10 scale)
- Migraine frequency and duration (if applicable)
- Activities limited by light sensitivity
- Environments most and least challenging
This provides objective data on whether FL-41 is providing benefit and helps guide adjustments.
When FL-41 Is Not Enough
If consistent FL-41 wear over 6–12 weeks does not provide meaningful improvement, this typically indicates that:
- The underlying condition needs more aggressive treatment — Migraine prevention (CGRP inhibitors, topiramate, amitriptyline) or dry eye treatment may be needed before full FL-41 benefit is realized
- Dark adaptation has occurred from previous dark sunglass use — Gradual reversal under specialist guidance is needed
- The photophobia is of a type that responds less to spectral filtering — Some forms of ocular photophobia (uveitis, acute glaucoma) respond better to treatment of the underlying condition than to eyewear
- A different lens tint may be better — Some patients respond better to darker FL-41, Harmony lenses (a different rose tint), or conditioned tints
Explore all photophobia treatment options →
Frequently Asked Questions
Are FL-41 glasses covered by insurance? In the United States, FL-41 prescription lenses may be covered by vision insurance as prescription lenses (coverage for the prescription component, not the therapeutic tint specifically). Medical insurance coverage for FL-41 as a photophobia treatment is not standard but is sometimes obtained with documentation of medical necessity (physician letter, ICD-10 H53.14). Flexible Spending Accounts (FSA) and Health Savings Accounts (HSA) can typically be used for FL-41 lenses as prescribed medical devices.
Can I wear FL-41 while driving? Yes — FL-41 lenses are appropriate for daytime driving. The ~35–40% transmission is similar to light tint driving sunglasses and does not impair vision for driving. Do not drive at night in any tinted lenses that reduce overall light transmission.
Can children wear FL-41 glasses? Yes — the original clinical evidence was established in children. FL-41 is safe for children with pediatric migraine, photophobia from any cause, or light sensitivity in autism. Polycarbonate lenses are recommended for children.
How long do FL-41 lenses last? The FL-41 tint is applied to the lens material and does not fade under normal use. The lenses last as long as standard prescription lenses — typically 1–2 years before prescription change or frame wear necessitates replacement.
Sources
- Good PA, et al. “Tinted spectacles in childhood migraine.” Developmental Medicine and Child Neurology. 1991;33(11):977-980.
- Blackburn MK, et al. “FL-41 tint improves blepharospasm in patients with benign essential blepharospasm.” Ophthalmology. 1991;98(5):716-718.
- Katz BJ, Digre KB, et al. “Relief of photophobia in patients with migraine using FL-41 tinted spectacles.” Headache. 2010;50(4):674-679.
- Stringham JM, et al. “Macular pigment optical density and color discrimination in FL-41 tint wearers.” Experimental Eye Research. 2013;116:27-32.
- Noseda R, et al. “A neural mechanism for exacerbation of headache by light.” Nature Neuroscience. 2010;13(2):239-245.
- Noseda R, Burstein R. “Migraine photophobia originating in cone-driven retinal pathways.” Brain. 2016;139(7):1971-1986.
- Digre KB, Brennan KC. “Shedding light on photophobia.” Journal of Neuro-Ophthalmology. 2012;32(1):68-81.
- Katz BJ, Digre KB. “Diagnosis, pathophysiology, and treatment of photophobia.” Survey of Ophthalmology. 2016;61(4):466-477.