Concussion and Light Sensitivity: Causes, Duration & Recovery
Light sensitivity is one of the most common concussion symptoms. Learn why TBI causes photophobia, how long it lasts, and the most effective recovery strategies.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- 1. How Common Is Light Sensitivity After Concussion?
- 2. Two Phases of Post-Concussion Photophobia
- 3. Key Statistics on Concussion and Light Sensitivity
- 4. Why Does Concussion Cause Light Sensitivity?
- 5. Symptoms Beyond Light Sensitivity
- 6. How Long Does Concussion Light Sensitivity Last?
- 7. Diagnosis and Assessment
- 8. Treatment and Recovery Strategies
- 9. Return to School and Work: Accommodations
- 10. Post-Concussion Syndrome vs. Prolonged TBI Recovery
- 11. Related Conditions to Consider
- 12. When to Seek Medical Evaluation
- 13. Frequently Asked Questions
- 14. Sources
- Light sensitivity affects 43–58% of concussion patients acutely; 10–25% develop persistent post-concussion photophobia lasting months to years.
- Concussion photophobia results from thalamic sensitization and disrupted retino-thalamic signaling, not structural eye damage.
- FL-41 tinted lenses are the first-line eyewear intervention; neuro-optometric rehabilitation addresses the visual processing component.
- Prolonged rest in total darkness is counterproductive — controlled, graduated light exposure is part of evidence-based recovery.
- Persistent post-concussion photophobia beyond 4 weeks warrants specialist evaluation (neurologist, neuro-ophthalmologist, neuro-optometrist).
How Common Is Light Sensitivity After Concussion?

Light sensitivity (photophobia) is one of the most frequently reported — and most functionally disabling — symptoms following concussion and traumatic brain injury (TBI). Research consistently shows it affects 43–58% of concussion patients in the acute phase, with a significant subset experiencing persistent photophobia as part of post-concussion syndrome (PCS).
For many patients, photophobia is more disabling than headache. It makes it impossible to work in standard office lighting, attend school, drive a car, use a computer or phone, or even spend time outdoors. When light sensitivity persists for months or years — as it does for a substantial minority of concussion patients — it can reshape a person’s entire life.
Understanding why concussion causes photophobia, how long it typically lasts, and what evidence-based strategies accelerate recovery is essential for every concussion patient and their care team.
Two Phases of Post-Concussion Photophobia
Light sensitivity after concussion presents in two distinct phases:
Acute phase (0–14 days): Nearly universal immediately following concussion. The brain is in an acute neurometabolic crisis — glucose demand surges while blood flow decreases, creating cellular energy deficits. All sensory processing is amplified during this window. Photophobia in the acute phase is expected and typically begins to improve with appropriate rest.
Post-concussion syndrome (PCS) phase (beyond 14 days): When photophobia persists beyond two weeks, it suggests that underlying neurological disruption has not fully resolved. PCS-phase photophobia is driven by different mechanisms than acute photophobia and requires a different management approach. It can persist for months or, in some cases, years.
Key Statistics on Concussion and Light Sensitivity
- 43–58% of concussion patients experience significant photophobia
- Photophobia is among the top 5 most reported post-concussion symptoms alongside headache, cognitive fog, dizziness, and sleep disturbance
- In children and adolescents, photophobia may persist longer than in adults and is a significant predictor of prolonged recovery
- Patients with pre-existing migraine are significantly more likely to develop persistent post-concussion photophobia
- Visual symptoms (including photophobia, blurred vision, and difficulty reading) are present in up to 69% of concussion patients at initial evaluation
- Women are more likely than men to report persistent photophobia following concussion, possibly related to hormonal influences on pain processing
Read about other causes of light sensitivity →
Why Does Concussion Cause Light Sensitivity?
Concussion disrupts multiple neurological systems simultaneously, each contributing to photophobia through distinct but overlapping mechanisms. This multi-system disruption is why post-concussion photophobia can be so refractory to simple treatments.
1. Axonal Injury and Disrupted Neural Pathways
Concussion causes diffuse axonal injury — the stretching, shearing, or rupturing of neuronal axons throughout the brain. The visual system is particularly vulnerable because it involves long-range connections from the retina, through the optic nerve and optic tract, to the lateral geniculate nucleus, and ultimately to the visual cortex and associated areas.
When these axonal pathways are disrupted, visual signal processing becomes dysrhythmic and inefficient. The brain struggles to process normal light input, and the result is that ordinary light levels trigger an excessive neural response experienced as pain or overwhelming discomfort.
2. Thalamocortical Dysrhythmia

The thalamus is the brain’s sensory gatekeeper. In normal function, it filters incoming sensory signals — selecting what reaches conscious awareness and suppressing the rest. After TBI, thalamic neurons lose their normal oscillatory rhythms, a condition called thalamocortical dysrhythmia.
This dysrhythmia means the thalamus no longer properly gates sensory input. Stimuli that would normally be filtered — including ambient light — reach the cortex at full intensity, overwhelming it. Patients describe this as feeling “assaulted” by normal sensory environments that others find perfectly comfortable.
3. Autonomic Nervous System Dysfunction
The autonomic nervous system (ANS) controls many involuntary physiological functions, including the pupillary light reflex — the constriction of the pupil in response to light to protect the retina. After concussion, ANS dysfunction is extremely common, and the pupillary light reflex may become sluggish, asymmetric, or dysregulated.
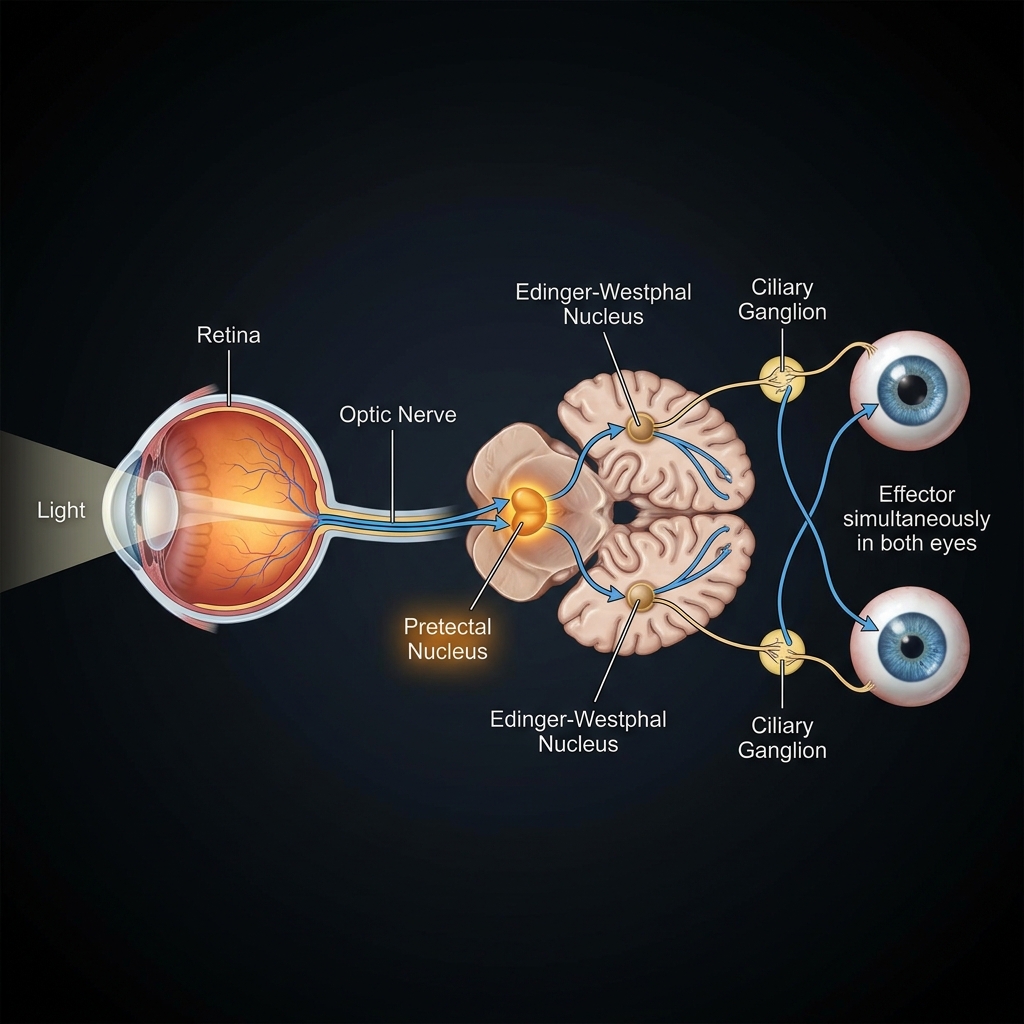
When the pupil fails to constrict appropriately in response to bright light, more light than normal reaches the retina. This over-stimulation contributes directly to photophobia. Additionally, ANS dysfunction in concussion is associated with postural orthostatic tachycardia (POTS)-like symptoms, which can include light sensitivity as part of the broader dysautonomia picture.
Read about POTS and light sensitivity →
4. Neuroinflammation
The mechanical forces of concussion initiate a neuroinflammatory cascade. Glial cells (microglia and astrocytes) become activated, releasing inflammatory cytokines throughout the brain. This neuroinflammation sensitizes neurons in the visual pathways, the trigeminal system, and the pain-modulating circuits — all of which contribute to photophobia.
Neuroinflammation may persist for weeks to months after the initial injury, explaining why some patients continue to experience photophobia long after conventional recovery timelines suggest they should be asymptomatic.
5. Post-Traumatic Migraine
Concussion frequently triggers post-traumatic headache (PTH), and in the majority of cases, PTH has the clinical features of migraine — including photophobia, phonophobia, nausea, and light-triggered pain. If a patient had an underlying migraine predisposition (which may have been subclinical), concussion often unmasks and exacerbates it.
Post-traumatic migraine adds a full migraine-mediated photophobia mechanism on top of the concussion-specific neurological disruption — making management more complex and requiring migraine-specific treatment alongside concussion care.
6. Oculomotor Dysfunction
Beyond photophobia per se, concussion frequently disrupts the oculomotor system — the neural networks controlling eye movement, tracking, convergence, and accommodation. These dysfunctions (convergence insufficiency, accommodative spasm, saccadic dysfunction) make any form of visual activity — including reading, screen use, and navigating a visually busy environment — intensely uncomfortable. While distinct from photophobia, oculomotor dysfunction and photophobia commonly coexist and compound each other.
Read about how eyes are affected by light sensitivity →
Symptoms Beyond Light Sensitivity
Post-concussion photophobia rarely occurs in isolation. Understanding the full symptom picture helps target treatment more effectively:
- Headache — present in over 90% of acute concussion patients; often migraine-phenotype
- Phonophobia (noise sensitivity) — closely linked to photophobia; shares the same thalamocortical dysrhythmia mechanism
- Cognitive fog — difficulty concentrating, word-finding problems, memory impairment
- Dizziness and vestibular dysfunction — balance problems often worsened by visual stimuli
- Screen intolerance — inability to use digital devices; combines photophobia with oculomotor strain
- Sleep disturbance — insomnia or hypersomnia; disrupted circadian rhythm
- Anxiety and depression — both develop secondary to chronic symptoms and disability
- Reading difficulty — convergence insufficiency and accommodative dysfunction make reading painful
- Visual motion sensitivity — discomfort in visually busy environments (busy patterns, scrolling, moving crowds)
Read about light and sound sensitivity →
How Long Does Concussion Light Sensitivity Last?
Recovery timelines vary significantly based on patient age, injury severity, pre-existing conditions, and adherence to appropriate management:
| Population | Typical Recovery Timeline |
|---|---|
| Children (ages 5–12) | 4–6 weeks on average |
| Teenagers | 4–8 weeks; can extend significantly |
| Adults (sports concussion, no prior history) | 1–4 weeks |
| Adults with pre-existing migraine | 6–12 weeks or longer |
| Adults with PCS | 3–12 months; occasionally years |
| Severe TBI | Permanent in some cases |
| Repeat concussions | Progressively longer recovery |
Factors Predicting Slower Recovery
- Prior concussion history — the most consistent predictor of prolonged recovery
- Pre-existing migraine — dramatically increases risk of PCS with photophobia
- Pre-existing anxiety or depression — amplifies all PCS symptoms via central sensitization
- Female sex — associated with longer recovery in multiple studies
- Younger age (teens) — developing brains are more vulnerable to prolonged disruption
- High-acuity initial symptoms — severe acute photophobia predicts longer recovery
- Inappropriate management — complete dark rest (outdated approach) worsens outcomes; controlled activity is now recommended
Diagnosis and Assessment
Concussion is a clinical diagnosis — no imaging test reliably detects it. CT and MRI are normal in the vast majority of concussions. Assessment is based on symptom history, neurological examination, and standardized tools.
Standard Assessment Tools
- SCAT6 (Sport Concussion Assessment Tool 6) — includes photophobia and phonophobia as standard symptom items
- PCSS (Post-Concussion Symptom Scale) — 22-item scale rating symptom severity; photophobia is a specific item
- VOMS (Vestibular/Ocular Motor Screening) — assesses vestibular and visual dysfunction contributing to photophobia
- Pupillometry — quantitative assessment of pupillary light reflex; may detect ANS dysfunction contributing to photophobia
Visual System Examination
A comprehensive vision assessment is recommended for concussion patients with significant photophobia:
- Near point of convergence (NPC) — assesses convergence insufficiency
- Smooth pursuit and saccades — oculomotor tracking quality
- Accommodation assessment — near-far focusing speed
- Pupillary light reflex — speed and symmetry of pupil response
Treatment and Recovery Strategies
Phase 1: Acute Management (Days 1–7)
Relative rest, not complete darkness. Current guidelines have moved away from recommending complete darkness and strict light avoidance. The 2023 Concussion in Sport Group consensus and similar guidelines now recommend relative rest — avoiding activities that significantly worsen symptoms, while allowing light activity that does not aggravate symptoms.
Complete darkness promotes dark adaptation, making the eyes increasingly sensitive to any light and worsening long-term photophobia. Instead:
- Reduce, but do not eliminate, light exposure
- Use FL-41 tinted lenses — these filter problematic wavelengths without promoting dark adaptation
- Dim lighting to a comfortable level rather than total blackout
- Avoid screens in the first 24–48 hours, then reintroduce gradually at reduced brightness
FL-41 glasses are the most appropriate eyewear for acute concussion photophobia:
- Specifically filter the wavelengths most associated with photophobia and migraine
- Light enough not to cause dark adaptation
- Can be worn continuously without worsening long-term sensitivity
- Available without prescription for immediate use during recovery
Avoid dark sunglasses indoors. This is a critical and counterintuitive point. Dark sunglasses worn indoors cause dark adaptation — the visual system adjusts to low light, making sensitivity to any light increase progressively. This is one of the most common management mistakes and can significantly prolong photophobia.
Phase 2: Active Rehabilitation (Weeks 2–12)
Vision therapy is among the most evidence-supported interventions for post-concussion visual dysfunction, including photophobia:
- Convergence therapy exercises for convergence insufficiency
- Saccadic training
- Accommodation exercises
- Visual tracking rehabilitation
- Brock string and other binocular vision exercises
Neuro-optometric rehabilitation — provided by optometrists with specialized TBI training — addresses the full spectrum of visual dysfunction beyond standard ophthalmology or optometry.
Vestibular therapy — if vestibular dysfunction (dizziness, balance problems, visual motion sensitivity) co-occurs with photophobia, vestibular physical therapy is essential. Visual and vestibular symptoms in concussion are deeply interconnected.
Gradual aerobic exercise. The evidence-based Buffalo Concussion Treadmill Test (BCTT) protocol prescribes sub-threshold aerobic exercise as soon as the acute phase allows. Controlled aerobic exercise promotes neuroplasticity, reduces neuroinflammation, and improves autonomic function — all of which contribute to photophobia reduction. Counterintuitively, careful controlled exercise accelerates recovery better than prolonged rest.
Light desensitization. For persistent photophobia, structured, gradual light exposure programs — supervised by a neuropsychologist or neuro-optometrist — can help retrain the visual system’s tolerance. This involves controlled, progressive exposure to increasing light levels in therapeutic settings.
Medication Options
For post-concussion syndrome with persistent photophobia, several medications have evidence:
Amitriptyline or nortriptyline (low-dose, 10–25 mg at bedtime): The most commonly prescribed medications for PCS. They reduce central sensitization, improve sleep, and reduce headache frequency. Often provide modest photophobia relief.
Gabapentin or pregabalin: For neuropathic pain and central sensitization components of PCS; may reduce photophobia indirectly by reducing general neural hyperexcitability.
CGRP inhibitors (erenumab, fremanezumab, galcanezumab): If post-traumatic migraine is contributing to photophobia, CGRP pathway treatments may be appropriate. Increasingly used in PCS patients with a migraine phenotype.
Melatonin (0.5–3 mg at bedtime): Supports the sleep disruption common in PCS and may have additional neuroprotective effects. Well-tolerated.
Magnesium glycinate (400 mg daily): Anti-inflammatory and neuromodulatory effects; some evidence for reducing headache and photophobia in post-traumatic headache.
Note: No medications are FDA-approved specifically for post-concussion syndrome. All pharmacological choices should be made with a physician.
Environmental and Screen Modifications
Lighting adjustments:
- Replace fluorescent overhead lighting (which flickers and contains disproportionate blue-wavelength light) with warm LED bulbs (2700–3000K)
- Use dimmable lighting controls throughout home and workspace
- Position workspaces away from windows with direct sunlight
- Use window films or cellular blinds to control natural light
Screen management:
- Enable dark mode and night mode on all devices
- Reduce brightness to the minimum comfortable level
- Increase text size to reduce visual strain from dense reading
- Increase font contrast to reduce accommodative effort
- Use screen reading software where possible to reduce visual load
- Take mandatory breaks from screens every 20 minutes
Vehicle considerations: Bright changing outdoor light during car travel is a significant photophobia trigger. In most states, photophobia patients can obtain a medical exemption for darker window tint — something most patients never know is available.
Full guide: Screen use and light sensitivity →
Return to School and Work: Accommodations
Photophobia is a legitimate disability in academic and workplace settings, and formal accommodations can make an enormous difference:
Academic Accommodations
- Extended time on tests and assignments
- Ability to use reduced lighting or individual lighting
- Permission to use printed materials instead of screens
- Access to audio recordings of lectures
- Rest breaks during class
- Exemption from gym/PE during acute recovery
- Permission to wear tinted lenses in class
- Online or remote attendance during recovery
Workplace Accommodations
- Work-from-home or remote work options
- Desk positioned away from windows
- Individual lighting control (desk lamp rather than overhead fluorescents)
- Anti-glare screen filters for monitors
- Flexible hours to avoid peak light conditions
- Reduced screen time with alternative workflows
- Formal ADA accommodation documentation from a physician
Guide to living with light sensitivity →
Post-Concussion Syndrome vs. Prolonged TBI Recovery
It is important to distinguish post-concussion syndrome (PCS) from the recovery trajectory of more severe traumatic brain injuries:
PCS refers specifically to the persistence of concussion symptoms (including photophobia) beyond the expected recovery window (typically 10–14 days for adults, 4 weeks for adolescents) following a mild TBI. Photophobia in PCS tends to be manageable and often improves with appropriate treatment.
Moderate to severe TBI can cause structural brain damage visible on MRI, with correspondingly more severe and potentially permanent visual and photophobic symptoms. Management requires a multidisciplinary neurorehabilitation team.
Related Conditions to Consider
Concussion photophobia frequently coexists with or overlaps with:
Migraine and light sensitivity — post-traumatic migraine is the most common headache type following concussion
Anxiety and light sensitivity — anxiety both amplifies photophobia and develops secondary to chronic PCS symptoms
POTS and light sensitivity — dysautonomia following concussion can manifest with POTS symptoms including light sensitivity
Dry eye and light sensitivity — concussion can disrupt corneal innervation and reduce blink rate, contributing to dry-eye-based photophobia
Sound and light sensitivity — phonophobia almost universally accompanies post-concussion photophobia
When to Seek Medical Evaluation
See your doctor or neurologist if:
- Photophobia has not improved after 2 weeks
- Symptoms are worsening rather than improving
- New symptoms develop (vision changes, escalating headache severity, vomiting)
- Photophobia is preventing return to normal daily activities
- You have had previous concussions
Emergency warning signs — go to the ER immediately:
- Sudden severe headache (“worst of your life”) — may indicate hemorrhage
- One pupil significantly larger than the other
- Loss of consciousness or inability to be woken
- Repeated vomiting after the immediate injury period
- Seizure
- Progressive confusion or deteriorating mental status
- Weakness, numbness, or loss of coordination
Read more about photophobia as a medical emergency →
Frequently Asked Questions
Is photophobia after concussion permanent? For most patients with a single uncomplicated concussion, photophobia resolves within weeks to months with appropriate management. Persistent photophobia lasting more than a year is more common in those with prior concussion history, pre-existing migraine, or inadequate rehabilitation.
Should I stay in a dark room after a concussion? No. Current evidence recommends relative rest — reducing but not eliminating light — rather than complete darkness. Complete darkness promotes dark adaptation and prolongs photophobia recovery. Use FL-41 tinted lenses instead to manage discomfort while maintaining some light exposure.
Can I use screens if I have post-concussion photophobia? Brief, low-brightness screen use is generally acceptable once the acute phase (48–72 hours) has passed. Use dark mode, minimum brightness, and take breaks every 20 minutes. Completely avoiding screens often prolongs recovery by eliminating important visual system stimulation needed for neuroplasticity.
Does photophobia mean my concussion was severe? Not necessarily. Even mild concussions cause significant photophobia. Photophobia severity does not reliably predict injury severity. Its persistence, however, may predict recovery duration.
Can green light help with post-concussion photophobia? Narrow-band green light (520 nm) is uniquely tolerated because of its minimal ipRGC activation. Some patients find green-tinted environments or green light therapy more comfortable than other light sources during concussion recovery, though clinical evidence in TBI specifically is limited.
Sources
- Master CL, et al. “Vision diagnoses are common after concussion in adolescents.” Clinical Pediatrics. 2016;55(3):260-267.
- Leddy JJ, et al. “Rehabilitation of Concussion and Post-concussion Syndrome.” Sports Health. 2012;4(2):147-154.
- Waddell ML, et al. “Photosensitivity in post-concussion syndrome.” Journal of Neuro-Ophthalmology. 2021.
- Bohnen N, et al. “Post-traumatic and emotional factors in light sensitivity after mild head injury.” Acta Neurologica Scandinavica. 1992.
- Silverberg ND, et al. “Management of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice Guidelines.” Archives of Physical Medicine and Rehabilitation. 2020;101(2):382-393.
- Ventura RE, et al. “Diagnostic criteria for post-COVID-19 condition: a Delphi consensus study.” The Lancet Infectious Diseases. 2021.
- Ellis MJ, et al. “Visual dysfunction following sports-related concussion.” Current Neurology and Neuroscience Reports. 2017;17(6):53.
- Kontos AP, et al. “Light sensitivity in the acute period following sport-related concussion.” Journal of Athletic Training. 2020.
- McCrory P, et al. “Consensus statement on concussion in sport — the 6th International Conference on Concussion in Sport.” British Journal of Sports Medicine. 2023.