Photophobia (Light Sensitivity): The Complete Guide
What is photophobia? Learn about light sensitivity causes, symptoms, related conditions, and effective treatments in this comprehensive, expert-reviewed guide.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- 1. What Is Photophobia?
- 2. How Common Is Photophobia?
- 3. The Neuroscience: How Light Sensitivity Works
- 4. What Causes Photophobia?
- 5. Symptoms of Photophobia
- 6. Measuring and Classifying Photophobia Severity
- 7. How Is Photophobia Diagnosed?
- 8. Treatment Options
- 9. Photophobia in Specific Conditions
- 10. When Is Photophobia a Medical Emergency?
- 11. Photophobia vs. Photosensitivity
- 12. Frequently Asked Questions
- 13. Sources
- Photophobia is a neurological symptom, not a disease — it signals an underlying condition affecting 17–20% of the population.
- 80–90% of migraine sufferers experience photophobia; it is also common in concussion, dry eye, MS, and autoimmune disorders.
- Blue light (450–480 nm) triggers the most discomfort; green light (~520 nm) is uniquely tolerable and may reduce pain.
- FL-41 tinted lenses and treating the underlying condition are the most evidence-backed management strategies.
- Wearing dark sunglasses indoors worsens photophobia over time through dark adaptation — use FL-41 tints instead.
What Is Photophobia?

Photophobia — commonly known as light sensitivity — is a condition where normal or even low levels of light cause discomfort, pain, or an overwhelming need to squint or close the eyes. Despite its name (literally translated as “fear of light” from Greek phōs meaning light, and phobos meaning fear), photophobia is not a psychiatric phobia. It is a neurological and sensory symptom — an abnormal, uncomfortable response to light stimulation.
Photophobia is not a disease in itself. It is a symptom — a signal that something else is happening in the nervous system, the eyes, or elsewhere in the body. It can be associated with more than 30 distinct medical conditions, ranging from everyday problems like dry eyes to serious neurological emergencies like meningitis. Understanding what photophobia is, what causes it, and what can be done about it is the first step toward effective management.
The experience of photophobia varies enormously from person to person. Some people find bright sunlight uncomfortable but manage it easily with sunglasses. Others are unable to tolerate even dim indoor lighting, to the point where they must live and work in near-total darkness. Between these extremes lies a wide spectrum of severity, and most people with chronic photophobia fall somewhere in the middle — managing day to day while making significant lifestyle accommodations to avoid painful light exposure.
How Common Is Photophobia?
Light sensitivity is far more common than most people realize. It is not a rare or exotic condition — it is a mainstream medical symptom affecting millions worldwide:
- Approximately 17–20% of the general population experiences some degree of chronic light sensitivity
- 80–90% of migraine sufferers experience photophobia during attacks, making it one of the hallmark symptoms of migraine
- 40–60% of migraineurs have interictal photophobia — persistent light sensitivity between migraine attacks even when headache-free
- Up to 50% of people with concussion experience significant photophobia during recovery
- Light sensitivity is more common in people with lighter-colored eyes due to lower melanin density in the iris
- Photophobia affects all age groups, though specific causes vary: dry eye is more prevalent in older adults, while migraine photophobia is most common among adults aged 18–55
Read more about who gets photophobia and why →
The Neuroscience: How Light Sensitivity Works
To understand photophobia, it helps to understand how the brain processes light signals and why that process can go wrong.
How Normal Light Processing Works
When light enters the eye, it triggers signals from photoreceptors (rods and cones) in the retina. These signals travel through the optic nerve to the visual cortex at the back of the brain, where they are processed into the images we see. In normal conditions, this process is seamless and does not cause pain.
The Role of Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs)

Beyond rods and cones, the retina contains a specialized third type of light-sensing cell: intrinsically photosensitive retinal ganglion cells (ipRGCs) . Unlike regular photoreceptors, ipRGCs contain a photopigment called melanopsin and are particularly sensitive to short-wavelength (blue) light. They project signals not only to the visual cortex, but also directly to the thalamus — a deep brain structure involved in sensory relay and pain processing.
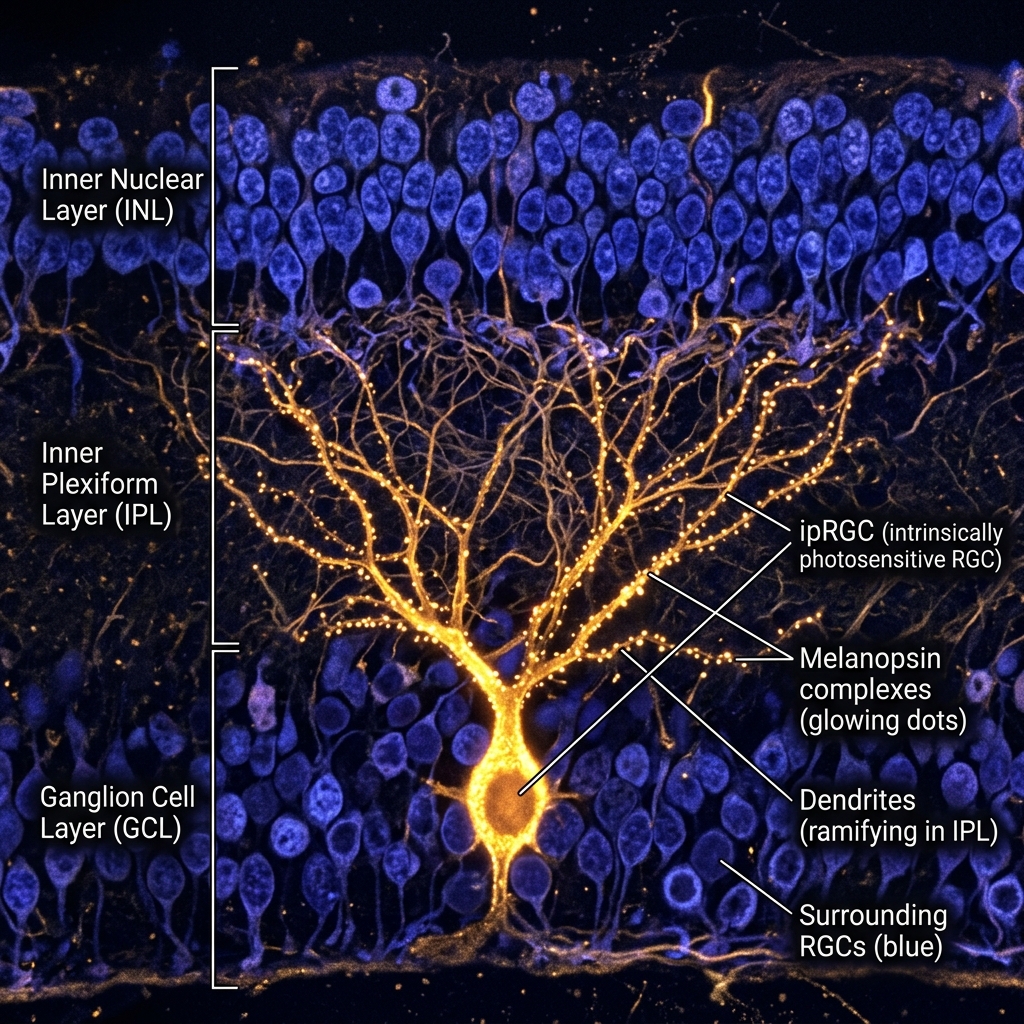
This thalamic projection is critical to understanding photophobia. Research by Dr. Rami Burstein and colleagues at Harvard Medical School demonstrated that in photophobic states — particularly during migraine — the thalamic neurons receiving ipRGC input become hypersensitized. Normal levels of light that would usually produce no pain become amplified into genuinely painful signals.
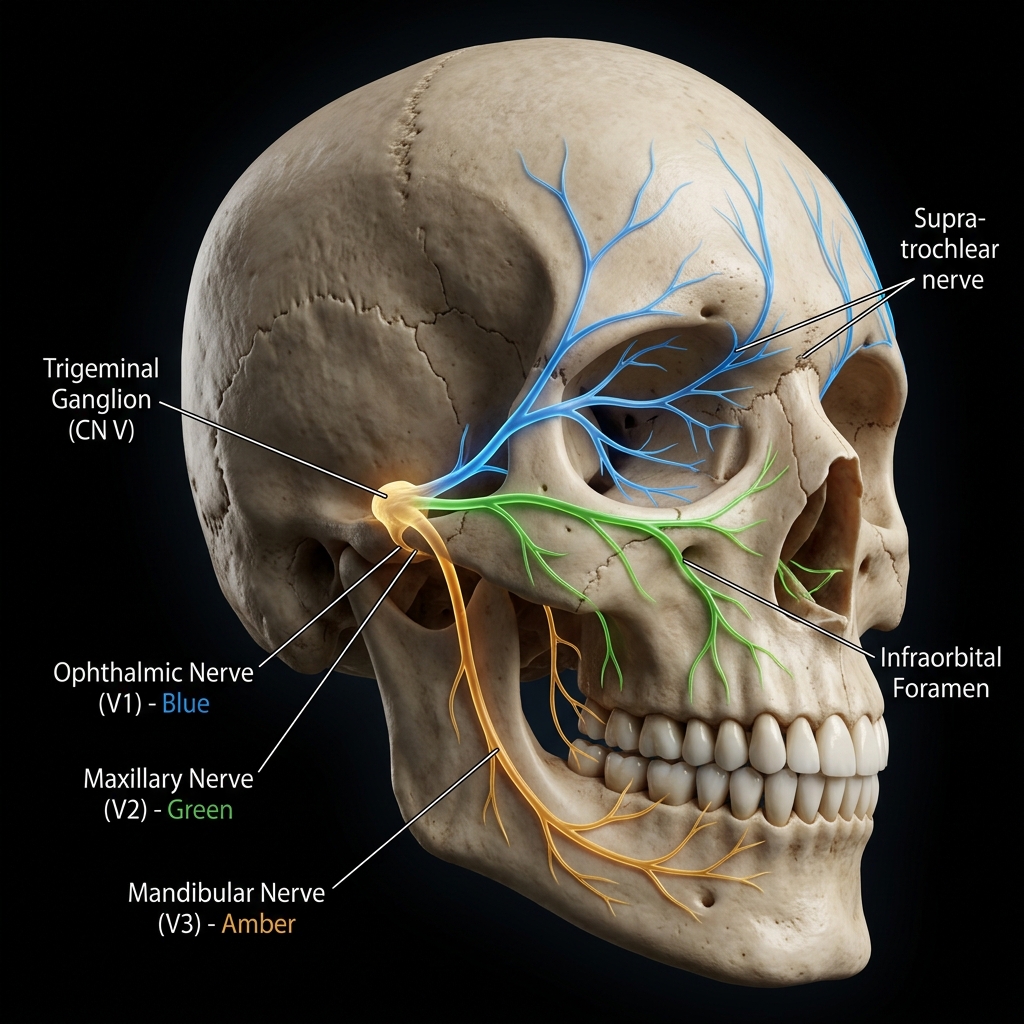
The Trigeminal Connection
The trigeminal nerve — the largest cranial nerve, responsible for sensation from the face, head, and eyes — plays a central role in photophobia. In conditions like migraine and concussion, the trigeminal nerve becomes sensitized (a process called central sensitization). When sensitized, it amplifies all incoming sensory signals, including those from light, making normal light genuinely painful rather than merely uncomfortable.
Why Different Wavelengths Hurt Differently
Not all light is equally painful in photophobic states. Research shows that:
- Blue light (450–480 nm) is most strongly activating for ipRGCs and tends to cause the most discomfort
- Red and amber light are less activating and therefore better tolerated
- Green light (around 520 nm) is uniquely tolerated — and may even reduce pain — because it activates a different, less sensitized pathway
This wavelength-specific sensitivity is the scientific rationale behind FL-41 tinted lenses, which filter blue and amber wavelengths, and green light therapy, which exploits the tolerability of narrow-band green light.
Read about screen use and blue light sensitivity →
What Causes Photophobia?
Photophobia is a symptom, not a disease — meaning it always has an underlying cause. The causes span neurology, ophthalmology, pharmacology, dermatology, and psychiatry.
Neurological Causes
Neurological conditions are the most common source of chronic, recurring photophobia:
Migraine is the leading cause of episodic photophobia worldwide, affecting an estimated 1 billion people globally. Photophobia during migraine is so characteristic that it is an official diagnostic criterion. The mechanisms involve trigeminal sensitization, thalamic hypersensitivity, and ipRGC activation, as described above.
Concussion and traumatic brain injury (TBI) frequently cause post-traumatic photophobia, which can persist for weeks, months, or even years after the initial injury. The disruption of normal neural signaling in the brainstem and thalamus contributes to disordered light processing. Photophobia is among the most commonly reported and most disabling symptoms of post-concussion syndrome.
Meningitis — inflammation of the membranes surrounding the brain — causes photophobia as a classic diagnostic sign, alongside severe headache and neck stiffness. Bacterial meningitis is a medical emergency requiring immediate treatment.
Fibromyalgia — a chronic pain condition characterized by widespread sensitization — frequently includes heightened sensitivity to light, sound, and touch as part of its central sensitization profile.
Multiple sclerosis (MS) can cause photophobia through optic neuritis (inflammation of the optic nerve) or through lesions affecting visual processing pathways in the brain.
POTS (Postural Orthostatic Tachycardia Syndrome) — a dysautonomia condition — is associated with light sensitivity as part of a broader sensory processing dysregulation.
Vestibular migraine combines migraine with vestibular dysfunction, producing dizziness, balance problems, and visual sensitivity including photophobia.
View the complete list of conditions that cause light sensitivity →
Eye-Related Causes
Many eye conditions directly increase the eye’s sensitivity to light by exposing nerve endings on the cornea or disrupting normal ocular physiology:
Dry eye syndrome is an extremely common cause of photophobia. When the tear film is unstable or deficient, the corneal surface is inadequately lubricated, exposing corneal nerve endings to environmental stimulation including light. This is one of the most treatable causes of photophobia.
Corneal abrasions (scratches to the cornea) cause acute, severe photophobia due to direct exposure of corneal nociceptors (pain receptors). The cornea is the most densely innervated tissue in the body, containing up to 7,000 nerve endings per square millimeter.
Uveitis and iritis — inflammation inside the eye — cause photophobia because inflamed iris muscles spasm in response to light constriction (the pupillary light reflex). This spasm is intensely painful.
Conjunctivitis (pink eye, whether bacterial, viral, or allergic) causes corneal and conjunctival inflammation that results in significant photophobia, especially viral conjunctivitis.
Glaucoma — particularly acute angle-closure glaucoma — can cause severe photophobia alongside eye pain and vision changes. This is a medical emergency.
Read the full guide to eyes and light sensitivity →
Medication-Related Causes
More than 100 medications have photosensitivity as a known side effect:
- Doxycycline and other tetracycline antibiotics cause both skin photosensitivity and ocular photophobia
- Accutane (isotretinoin) — used for acne — commonly causes dry eyes, which secondarily produces photophobia
- Certain SSRIs (fluoxetine, sertraline) are associated with photosensitivity in some patients
- Hydroxychloroquine (Plaquenil) — used in lupus and rheumatoid arthritis — can cause retinal changes and photosensitivity
- Diuretics including hydrochlorothiazide increase sun sensitivity
- Amiodarone (a heart medication) causes significant photosensitivity in up to 75% of patients with long-term use
Browse the complete guide to drug-induced photosensitivity →
Autoimmune and Systemic Causes
Several systemic conditions produce photophobia through inflammation, nerve involvement, or skin-light reactions:
Lupus (SLE) causes both skin photosensitivity (rashes triggered by UV light) and ocular photophobia. The two are distinct mechanisms but can coexist in the same patient.
Lyme disease — particularly disseminated Lyme — can affect the nervous system and cause persistent photophobia.
Sjögren’s syndrome causes severe dry eyes as a primary feature, which leads to significant corneal-based photophobia.
Fibromyalgia and other central sensitization disorders amplify all sensory inputs including light.
Psychiatric and Psychological Factors
Anxiety disorders have a bidirectional relationship with photophobia. Anxiety can amplify the perception of light sensitivity through heightened arousal and sensory processing, while chronic photophobia itself causes anxiety and social isolation.
Depression is strongly associated with photophobia, and research suggests the serotonergic pathways involved in depression also play a role in light sensitivity regulation.
Autism spectrum disorder (ASD) — sensory processing differences in autism frequently include hypersensitivity to light as part of broader sensory dysregulation.
Read the full guide to causes of light sensitivity →
Symptoms of Photophobia
Light sensitivity does not always present the same way. The full symptom picture includes both primary ocular symptoms and secondary systemic effects:
Primary Symptoms
- Eye discomfort or pain in normally tolerable lighting — the defining symptom
- Squinting or involuntary eye closure (blepharospasm in severe cases)
- Excessive tearing (epiphora) — a reflex response to ocular irritation
- Brow ache from sustained squinting and frontalis muscle tension
- Blurred or disturbed vision in bright conditions
Secondary Symptoms
- Headache triggered or significantly worsened by light exposure
- Nausea in severe cases, particularly migraine-associated photophobia
- Irritability and mood changes during photophobic episodes
- Difficulty concentrating in environments that are too bright
- Avoidance behaviors — wearing sunglasses indoors, darkening rooms, limiting outdoor activity
Interictal Photophobia
An important and often overlooked phenomenon is interictal photophobia — persistent light sensitivity that occurs between episodes of the primary condition, not only during active flares. Research suggests that 40–60% of migraineurs experience some degree of persistent photophobia even when they are headache-free, likely due to ongoing thalamic sensitization.
Read the complete guide to light sensitivity symptoms →
Measuring and Classifying Photophobia Severity
Clinicians and researchers classify photophobia on a spectrum:
- Mild: Discomfort in very bright environments (direct sun, high-wattage overhead lighting) but functional in normal indoor settings
- Moderate: Discomfort in standard indoor lighting; manages with sunglasses or dimming; affects productivity and social activities
- Severe: Unable to tolerate most indoor lighting; significant disability; restricts daily activities
- Profound: Unable to tolerate any meaningful light; requires constant near-darkness; causes severe disability
A validated assessment tool, the 10-item Photosensitivity Assessment or the Visual Function Index (VFQ-25), may be used in clinical settings to track severity over time.
How Is Photophobia Diagnosed?
Because photophobia is a symptom rather than a diagnosis, the evaluation process aims to identify the underlying cause. There is no single “photophobia test.”
Who to See
- Ophthalmologist — for eye-related causes (dry eye, corneal conditions, uveitis, glaucoma)
- Neurologist or headache specialist — for migraine, concussion, or central sensitization
- Primary care physician — for initial evaluation and specialist referral
- Rheumatologist — for autoimmune causes (lupus, Sjögren’s)
- Physiatrist or neuropsychologist — for post-concussion photophobia
Evaluation Components
A thorough evaluation typically includes:
- Detailed medical and symptom history — when photophobia started, how long it lasts, what worsens or improves it, associated symptoms (headache, dizziness, vision changes), medication review
- Complete eye examination — tear film assessment (Schirmer’s test, TBUT), corneal examination with slit lamp, pupillary light reflex testing, intraocular pressure measurement
- Pupillary response evaluation — abnormal pupillary constriction in response to light may indicate iritis or uveitis
- Neurological evaluation — if a neurological cause is suspected, this may include brain imaging (MRI) to rule out structural causes or optic neuritis
- Bloodwork — ANA, anti-dsDNA, and other autoimmune markers if lupus or Sjögren’s is suspected
The Pupillary Light Reflex and Photophobia
Interestingly, research shows that in many photophobic patients, the pupil actually constricts more slowly and incompletely in response to light — the opposite of what might be expected. This suggests that photophobia is a supraspinal phenomenon (happening in the brain) rather than a simple peripheral reflex.
Treatment Options
Treatment for photophobia must address the underlying cause. There is no universal photophobia cure, but a wide range of interventions can significantly reduce symptoms.
Protective Eyewear
FL-41 tinted lenses are the most evidence-backed eyewear intervention for photophobia. This rose-pink tint was originally developed for patients with blepharospasm and fluorescent light sensitivity, and multiple studies have demonstrated that FL-41 lenses reduce both migraine frequency and light sensitivity in photophobic patients. They filter out the blue-green wavelengths (450–530 nm) that are most activating for ipRGCs.
Blue light blocking glasses filter high-energy visible blue light (415–455 nm) primarily emitted by screens. These may help with screen-related photophobia but do not provide the same therapeutic benefit as properly tuned FL-41 lenses for migraine-related photophobia.
Anti-glare glasses reduce reflected glare from polished surfaces, computer screens, and oncoming headlights, making them useful for driving-related photophobia and screen sensitivity.
Standard sunglasses are appropriate for outdoor use, but wearing dark sunglasses indoors can worsen photophobia over time by promoting dark adaptation — the eyes become more sensitive as they adapt to less light. Very dark tints should be reserved for outdoor use.
Compare all glasses options for light sensitivity →
Medical Interventions
Eye drops — artificial tears and lubricating drops are the first-line treatment for dry-eye-related photophobia. Prescription cyclosporine drops (Restasis, Cequa) reduce inflammatory dry eye. Dilating drops (atropine, cyclopentolate) may be used for iritis-related spasm.
Treating the underlying condition is the most effective long-term strategy. For migraine: triptans for acute attacks, CGRP inhibitors (Aimovig, Ajovy, Emgality) or topiramate for prevention. For uveitis: corticosteroid eye drops or systemic immunosuppressants. For dry eye: lubricants, punctal plugs, prescription drops, or warm compresses.
Green light therapy — exposure to narrow-band green light (520 nm) for 1–2 hours daily has shown promise in reducing migraine frequency and photophobia intensity in small clinical studies. Research by Dr. Mohab Ibrahim at the University of Arizona suggests green light activates natural pain-modulating pathways without activating photophobic ones.
Sunscreen and UV protection — for skin photosensitivity (as in lupus or drug-induced photosensitivity), broad-spectrum SPF is essential alongside photophobia management.
Browse all treatments for light sensitivity →
Lifestyle and Environmental Management
Lighting modifications at home and in the workplace can dramatically reduce photophobic exposure:
- Replace fluorescent lighting with incandescent or warm LED bulbs
- Use dimmable lighting controls
- Use bias lighting behind monitors to reduce screen-to-room contrast
- Use window films or blackout curtains to control natural light
Screen adjustments:
- Enable Night Mode / Warm Color temperature on all devices
- Reduce screen brightness to below ambient light levels
- Use the 20-20-20 rule: every 20 minutes, look at something 20 feet away for 20 seconds
- Consider using a matte screen protector to reduce glare
Read the full guide to living with light sensitivity →
The Window Tint Medical Exemption
An often-overlooked practical solution: photophobia patients in most U.S. states can qualify for a medical exemption for darker car window tint beyond the legal limit. This can make driving — and simply being in a car — dramatically more tolerable. Most patients never learn this option exists. A physician can provide an exemption letter documenting medical necessity.
Photophobia in Specific Conditions
Migraine
The most common cause. Photophobia during migraine involves thalamic sensitization and is bidirectional: light worsens migraine pain, and migraine causes photophobia. Full guide: Migraine and Light Sensitivity →
Concussion
Post-traumatic photophobia can be among the most persistent post-concussion symptoms, sometimes lasting years. Full guide: Concussion and Light Sensitivity →
Dry Eye
Dry eye is the most common and most treatable ocular cause of photophobia. Full guide: Dry Eye and Light Sensitivity →
Lupus
Lupus causes both skin-based photosensitivity and ocular photophobia through different mechanisms. Full guide: Lupus and Photosensitivity →
Drug-Induced
Over 100 medications list photosensitivity as a side effect. Full guide: Drug-Induced Photosensitivity →
Autism and Sensory Processing
Light sensitivity is a frequent component of sensory dysregulation in autism spectrum disorder. Full guide: Autism and Light Sensitivity →
When Is Photophobia a Medical Emergency?
Most photophobia is not an emergency — but some presentations require immediate medical evaluation:
Seek emergency care immediately if photophobia is accompanied by:
- Severe headache + stiff neck + fever — classic meningitis triad; bacterial meningitis is life-threatening
- Sudden vision loss — may indicate retinal detachment, acute glaucoma, or optic neuritis
- Severe eye pain with nausea and vomiting — possible acute angle-closure glaucoma (can cause permanent vision loss within hours if untreated)
- Following a head injury — even “mild” concussion with photophobia warrants evaluation
- Unilateral pupil dilation with new headache — possible aneurysm; call emergency services
Read more about meningitis and photophobia →
Photophobia vs. Photosensitivity
These terms are often used interchangeably but refer to distinct phenomena:
| Term | Definition | Primary System |
|---|---|---|
| Photophobia | Eye discomfort or pain in response to light | Neurological / Ocular |
| Photosensitivity | Abnormal skin reaction to sunlight (rash, burns) | Dermatological |
| Photic sensitivity | Brain’s hypersensitive response to visual stimuli (seizures) | Neurological |
Photophobia and photosensitivity can coexist in the same patient — this is particularly common in lupus, where both skin reactions to UV and eye discomfort from light are part of the disease picture.
Learn more about photophobia vs. photosensitivity terminology → Guide to skin photosensitivity →
Frequently Asked Questions
Is photophobia the same as light sensitivity? Yes. “Photophobia” is the medical term for light sensitivity. They describe the same symptom.
Can photophobia go away on its own? It depends on the cause. Photophobia from a corneal abrasion typically resolves within days as the injury heals. Photophobia from migraine may persist indefinitely but can be managed with treatment. Post-concussion photophobia often improves over months with appropriate management.
Why do I get a headache from bright lights? This is a hallmark of photophobia. Light activates sensitized thalamic neurons that are also part of the pain processing network. The result is that light exposure is processed as painful, triggering or worsening headache. This is most pronounced in migraine.
Should I wear sunglasses indoors if I have photophobia? Only dark glasses should be avoided for prolonged indoor use, as they promote dark adaptation and worsen photophobia over time. FL-41 tinted lenses, which are lighter in tint and specifically tuned to filter problematic wavelengths, are appropriate for extended indoor wear.
What is the best color light for photophobia? Green light at approximately 520 nm is the most tolerable and the least likely to trigger or worsen photophobic pain. Warm amber and red lighting are also better tolerated than blue, white, or cool LED lighting.
Can stress cause photophobia? Yes. Anxiety and stress can both trigger and worsen photophobia by increasing neural arousal and lowering the threshold for sensory discomfort. This is particularly relevant in anxiety disorder, depression, and fibromyalgia.
Sources
- Digre KB, Brennan KC. “Shedding light on photophobia.” Journal of Neuro-Ophthalmology. 2012;32(1):68-81.
- Noseda R, et al. “A neural mechanism for exacerbation of headache by light.” Nature Neuroscience. 2010;13(2):239-245.
- Katz BJ, Digre KB. “Diagnosis, pathophysiology, and treatment of photophobia.” Survey of Ophthalmology. 2016;61(4):466-477.
- Burstein R, et al. “Thalamic sensitization transforms localized pain into widespread allodynia.” Annals of Neurology. 2010;68(1):81-91.
- Ibrahim MM, et al. “Green light exposure induces pain relief and decreases inflammatory pain via endogenous opioid release.” Pain. 2021;162(7):1933-1942.
- Bhattacharya S, et al. “Photophobia: Mechanisms and treatments.” Current Neurology and Neuroscience Reports. 2020.
- Bernstein CA, et al. “Sensitization of the trigemino-vascular pathway: A review.” Cephalalgia. 2019;39(4):413-424.
- Hattar S, et al. “Melanopsin-containing retinal ganglion cells: architecture, projections, and intrinsic photosensitivity.” Science. 2002;295(5557):1065-1070.