Migraine and Light Sensitivity: Why It Happens & How to Manage It
Why do migraines cause light sensitivity? Learn the neuroscience behind migraine photophobia, how to manage it during attacks, and which treatments work best.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- 1. Why Migraines Cause Light Sensitivity
- 2. Migraine and Photophobia: Key Statistics
- 3. The Neuroscience: How Migraine Triggers Photophobia
- 4. How Severe Is Migraine Photophobia?
- 5. Interictal Photophobia: Between the Attacks
- 6. Migraine and Light as a Trigger: The Bidirectional Cycle
- 7. Migraine Variants and Their Light Sensitivity Profiles
- 8. Diagnosing Migraine Photophobia
- 9. Treatment Strategies for Migraine Photophobia
- 10. Related Conditions to Consider
- 11. When to See a Specialist
- 12. Sources
- 80–90% of migraine sufferers experience photophobia during attacks; 40–60% have persistent light sensitivity even between attacks.
- Migraine photophobia is driven by thalamic sensitization and trigeminal nerve hypersensitivity, not a simple eye problem.
- FL-41 tinted lenses are the most evidence-backed tool for managing migraine photophobia — dark sunglasses worn indoors worsen it.
- Treating migraine preventively (topiramate, amitriptyline, beta-blockers, CGRP antibodies) reduces both headache and interictal photophobia.
- Green light at ~520 nm is uniquely tolerable during migraine and may actively reduce pain intensity.
Why Migraines Cause Light Sensitivity

Light sensitivity (photophobia) is one of the most common, disabling, and diagnostically important symptoms of migraine — affecting an estimated 80–90% of migraine sufferers during attacks. It is so fundamental to the migraine experience that photophobia is an official diagnostic criterion under the International Classification of Headache Disorders (ICHD-3). For many people, light sensitivity is not just a symptom during attacks but a persistent, daily burden that reshapes how they live, work, and socialize.
This guide explains the neuroscience behind migraine photophobia, explores every variant of migraine-related light sensitivity, and provides a comprehensive evidence-based treatment overview. If you are struggling with migraine and light sensitivity, understanding the mechanisms at work is the foundation for finding effective relief.
Migraine and Photophobia: Key Statistics
The scale of the problem is significant:
- 80–90% of people with migraine experience photophobia during attacks
- 40–60% of migraineurs have persistent interictal photophobia between attacks even when pain-free
- Migraine affects approximately 1 billion people worldwide — making migraine-related photophobia one of the most prevalent forms of light sensitivity
- Photophobia is rated among the top three most disabling migraine symptoms, alongside head pain and nausea
- Women are three times more likely than men to experience migraine and its associated photophobia
- Up to 50% of migraine patients report that light is a direct trigger for their attacks — creating a vicious bidirectional cycle
Read more about what causes light sensitivity →
The Neuroscience: How Migraine Triggers Photophobia
Understanding why migraine causes such extreme light sensitivity requires looking inside the brain at the neural pathways involved. The mechanisms are complex and multifaceted, involving at least four interacting systems.
1. The Trigeminal Sensitization Pathway
The trigeminal nerve — the fifth and largest cranial nerve — is responsible for sensory sensation from the face, scalp, and eyes. During a migraine, inflammatory neuropeptides (including CGRP, substance P, and neurokinin A) are released from trigeminal nerve terminals, causing neurogenic inflammation and peripheral sensitization.
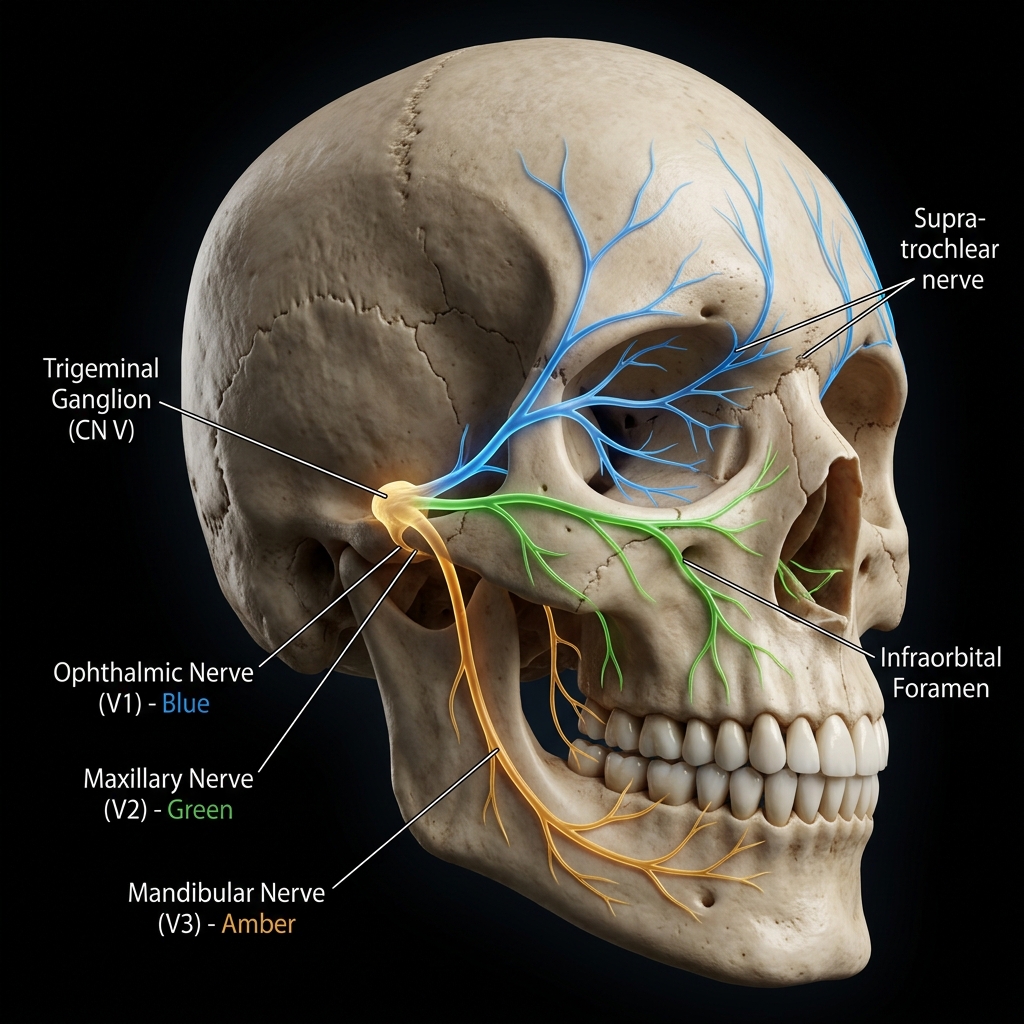
This peripheral sensitization then spreads centrally: the trigeminal nucleus caudalis (in the brainstem) and eventually higher brain centers become sensitized — a process called central sensitization. Once centrally sensitized, the nervous system amplifies all incoming sensory signals. Normal levels of light that would typically cause no pain are now processed as painful stimuli.
2. Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs)
The retina contains not only the well-known rods and cones but also a third type of light-detecting cell: intrinsically photosensitive retinal ganglion cells (ipRGCs) . These cells contain melanopsin, a photopigment maximally sensitive to blue-wavelength light (around 480 nm), and they project signals along a dedicated pathway to the thalamus and brainstem rather than the visual cortex.
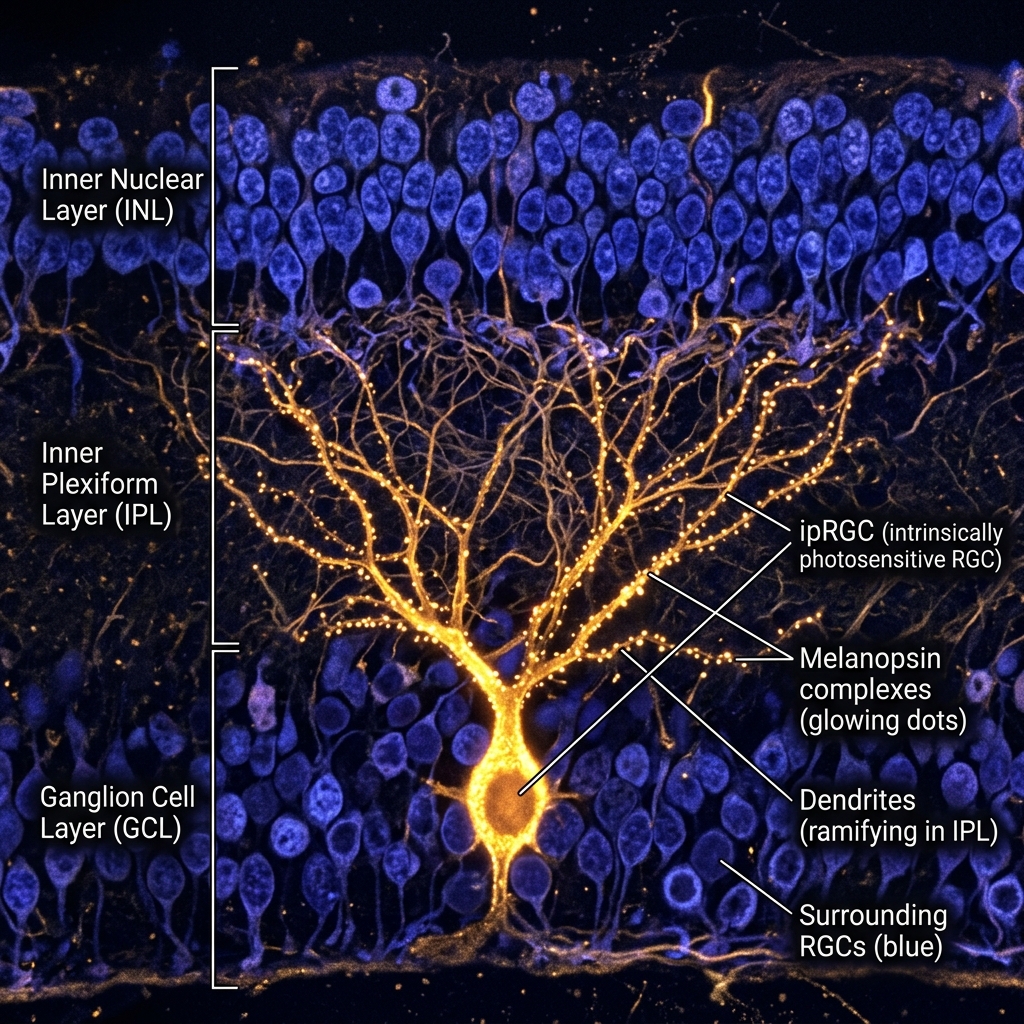
Crucially, this retino-thalamic pathway bypasses the normal visual processing centers and feeds directly into pain-modulating brain regions. Groundbreaking research by Dr. Rami Burstein and colleagues at Harvard Medical School demonstrated that in migraine, the thalamic neurons receiving ipRGC input become profoundly hypersensitized — making normal light input register as genuinely painful.
This research explained a phenomenon doctors had long observed: even congenitally blind individuals who lack functional rods and cones can still experience migraine photophobia, because their ipRGCs and the retino-thalamic pathway remain intact.
3. The Thalamic Pain Relay
The thalamus functions as the brain’s central “relay station” for sensory and pain signals. During migraine, thalamic neurons in the posterior thalamus become hyperexcitable and begin generating spontaneous pain signals amplified by any light input. This thalamic sensitization is why migraine photophobia can be so severe — even low levels of ambient light become intolerable because the thalamus is treating each light signal as a threat.
The thalamic connection also explains why photophobia can persist between migraine attacks (interictal photophobia) in many patients: the thalamus may remain in a partially sensitized state even when no active attack is occurring.

4. The Green Light Exception
One of the most clinically important discoveries in migraine neuroscience is that not all light is equally painful during a migraine:
- Blue light (450–480 nm) is the most activating for ipRGCs and causes the most photophobic pain
- White and cool-white light contain substantial blue-wavelength energy and are poorly tolerated
- Amber and red light are less activating and better tolerated
- Narrow-band green light (520–530 nm) is uniquely tolerated — and may actually reduce migraine pain — because it activates a smaller subset of ipRGCs that projects to pain-inhibiting rather than pain-amplifying thalamic neurons
This green light exception is the scientific foundation for FL-41 tinted lenses (which filter the most problematic wavelengths) and green light therapy (which harnesses the pain-reducing property of narrow-band green light).
Read the full guide to what causes photophobia →
How Severe Is Migraine Photophobia?
Light sensitivity during migraine exists on a spectrum, and understanding where your photophobia falls can guide treatment decisions:
Mild photophobia: Discomfort in bright outdoor sunlight or high-wattage fluorescent environments. Manageable with sunglasses outdoors. Most people can continue basic indoor activities.
Moderate photophobia: Discomfort in standard indoor lighting including office overhead lights and home lighting. Requires dimming rooms, avoiding fluorescent lights, and wearing tinted lenses for much of the day. Impacts work and social activities.
Severe photophobia: Unable to tolerate most indoor lighting at any level. Requires room darkening during attacks and significant light avoidance between attacks. Causes major disability — missed work, social isolation, inability to drive or use screens.
Profound photophobia: Complete inability to tolerate meaningful light at any time. Requires near-total darkness. This level is associated with the most severe forms of chronic migraine and can cause profound disability requiring medical intervention and often workplace accommodation.
Interictal Photophobia: Between the Attacks
One of the most underrecognized aspects of migraine is that photophobia does not only occur during attacks. Interictal photophobia — persistent light sensitivity between headaches when patients are technically “attack-free” — affects between 40–60% of migraineurs.

Interictal photophobia appears to result from ongoing thalamic sensitization that persists even after the acute attack resolves. The thalamus never fully “resets” to baseline sensitivity between attacks in many chronic migraineurs.
The clinical implications are significant:
- Patients are not imagining their between-attack light sensitivity
- Standard acute migraine treatments do not address interictal photophobia
- Daily prophylactic treatment (preventive medications or FL-41 lenses) is often needed
- Patients with interictal photophobia are often diagnosed with anxiety or depression because of their light avoidance, when the underlying driver is neurological
Migraine and Light as a Trigger: The Bidirectional Cycle
Light does not only worsen pain during an active migraine — it can also trigger the next migraine in susceptible individuals. Studies suggest up to 50% of migraine patients identify light as a trigger. Common triggering scenarios include:
- Fluorescent flickering — even at rates too fast for conscious perception (50–60 Hz)
- Bright sunlight, particularly with glare from reflective surfaces (snow, water, windshields)
- Sudden dark-to-bright transitions (entering a brightly lit store from outdoors)
- Screen glare — especially in darkened rooms where contrast between screen and environment is high
- Strobe or flashing lights — in entertainment venues, emergency vehicles, or certain video content
- Computer screens without blue light filtering during prolonged use
This creates a problematic bidirectional cycle: migraine causes photophobia, light exposure triggers migraines, and avoidance of light can ironically worsen long-term sensitivity through dark adaptation.
Migraine Variants and Their Light Sensitivity Profiles
Light sensitivity presents somewhat differently across migraine subtypes:
Migraine with Aura
Approximately 25–30% of migraineurs experience aura — transient neurological symptoms that typically precede the headache phase by 20–60 minutes. Visual aura (zigzag lines, scotoma, bright flashes) during the cortical spreading depression phase is accompanied by intense photophobia. The combination of visual disturbance and light sensitivity during aura can be particularly alarming. Full guide: Migraine with Aura and Light Sensitivity →
Chronic Migraine
Defined as 15 or more headache days per month (with at least 8 meeting migraine criteria), chronic migraine is almost universally associated with significant interictal photophobia. The degree of ongoing thalamic sensitization in chronic migraine patients makes normal daily light exposure consistently uncomfortable. Full guide: Chronic Migraine and Light Sensitivity →
Vestibular Migraine
Vestibular migraine combines migraine with vestibular dysfunction — producing dizziness, vertigo, and balance problems alongside headache or instead of it. Light sensitivity is extremely common in vestibular migraine and may be particularly triggered by moving visual environments (busy patterns, scrolling, visual motion in the periphery). Full guide: Vestibular Migraine and Light Sensitivity →
Ocular (Retinal) Migraine
Ocular migraine causes temporary monocular vision loss or visual disturbances in one eye, caused by reduced blood flow to the retina. Photophobia during and after an ocular migraine episode can be severe. Full guide: Ocular Migraine and Light Sensitivity →
Hemiplegic Migraine
This rare variant includes temporary weakness or paralysis on one side of the body during attacks, alongside severe photophobia and phonophobia. It requires specialized management.
Diagnosing Migraine Photophobia
Migraine is a clinical diagnosis — there is no definitive blood test or imaging finding. Diagnosis is based on symptom patterns meeting ICHD-3 criteria.
ICHD-3 diagnostic criteria for migraine without aura require at least 5 attacks with:
- Headache lasting 4–72 hours (untreated)
- At least 2 of: unilateral location, pulsating quality, moderate-severe intensity, aggravation by routine activity
- At least one of: nausea/vomiting, OR photophobia AND phonophobia
The presence of photophobia is thus central to the diagnostic picture. Notably, photophobia alone (without headache) during a suspected migraine episode does not rule out migraine — some patients have “silent migraine” where photophobia and other symptoms occur without significant head pain.
Red Flags Requiring Urgent Evaluation
Not all headache with photophobia is migraine. The following warrant urgent or emergency evaluation:
- Thunderclap headache (worst headache of life, reaching peak within seconds) — possible subarachnoid hemorrhage
- Headache + stiff neck + fever — possible meningitis (medical emergency)
- Photophobia + vision loss — possible retinal detachment or acute glaucoma
- New headache pattern in patients over 50 — possible temporal arteritis or intracranial pathology
- Progressively worsening headache over weeks — possible intracranial mass
Read more about photophobia emergencies →
Treatment Strategies for Migraine Photophobia
Effective management of migraine-related light sensitivity requires a layered approach addressing immediate relief, attack prevention, long-term desensitization, and environmental management.
Acute Attack Management
Environmental: At the onset of a migraine, moving to a dark, quiet room is consistently the most effective immediate intervention. Using blackout curtains or a sleep mask can significantly reduce photophobic pain. A cold compress over the eyes reduces blood vessel dilation and provides additional comfort.
Triptans (sumatriptan, rizatriptan, eletriptan, naratriptan, and others) are the most effective acute migraine medications and work by constricting dilated blood vessels and modulating trigeminal firing. They reduce photophobia alongside headache. Best taken early in the attack.
CGRP receptor antagonists (gepants: ubrogepant/Ubrelvy, rimegepant/Nurtec) are newer acute treatments that block the CGRP pathway — the primary inflammatory driver of migraine. They are particularly effective for patients who cannot take triptans.
NSAIDs (ibuprofen, naproxen sodium, aspirin) can be effective for mild-moderate migraine attacks and reduce associated photophobia. Most effective when taken early.
Antiemetics (metoclopramide, prochlorperazine) address nausea and also have mild analgesic properties that can complement migraine treatment.
Preventive (Prophylactic) Treatments
For patients with frequent attacks (4+ migraine days per month) or persistent interictal photophobia, preventive treatment is strongly recommended:
CGRP pathway preventives represent the most significant advance in migraine prevention in decades:
- Monthly injectables: erenumab (Aimovig), fremanezumab (Ajovy), galcanezumab (Emgality)
- Quarterly injectable: eptinezumab (Vyepti, IV infusion)
- Daily oral: atogepant (Qulipta) These drugs specifically block the CGRP molecule or its receptor, reducing both attack frequency and associated photophobia severity.
OnabotulinumtoxinA (Botox) — FDA-approved for chronic migraine only — involves 31 injections across the head and neck every 12 weeks. It reduces both headache days and interictal photophobia in many patients.
Traditional preventives including topiramate (Topamax), valproate, propranolol, amitriptyline, and venlafaxine have proven efficacy, though the newer CGRP drugs generally have better tolerability.
Magnesium supplementation (400–600 mg daily) has evidence for modest reduction in migraine frequency and photophobia in some patients, particularly those with aura. It is inexpensive and well-tolerated.
Riboflavin (Vitamin B2) at 400 mg daily has evidence for reducing migraine frequency through mitochondrial energy pathways.
Melatonin (3 mg nightly) has shown efficacy comparable to amitriptyline in some trials with excellent tolerability.
Eyewear Strategies
FL-41 tinted lenses are the most evidence-backed non-pharmacological intervention for migraine photophobia. The rose-pink FL-41 tint specifically filters blue-green wavelengths (450–530 nm) that are most activating for migraine-sensitized ipRGCs. Clinical studies demonstrate that FL-41 lenses:
- Reduce migraine attack frequency by 40–60% in some trials
- Significantly reduce interictal photophobia
- Allow patients to tolerate normal indoor environments more comfortably
- Are appropriate for daily wear without promoting dark adaptation (unlike dark sunglasses)
Blue light blocking glasses filter high-energy visible blue light from screens and may reduce screen-triggered migraine and associated photophobia in screen-heavy users.
Anti-glare glasses reduce specular glare from polished surfaces and screens — useful for driving and office environments.
Important: Dark sunglasses worn indoors promote dark adaptation, causing the eyes to become increasingly sensitive to light over time. This worsens long-term photophobia. FL-41 or other specifically-designed migraine lenses are preferred for indoor use.
Compare all glasses for migraine and light sensitivity →
Green Light Therapy
Research by Dr. Mohab Ibrahim at the University of Arizona has demonstrated that exposure to narrow-band green light (520 nm) for 1–2 hours daily may reduce migraine frequency and decrease photophobia intensity. Green light at this wavelength activates pain-inhibitory opioid pathways in the brain while producing minimal ipRGC activation — allowing a therapeutic effect without worsening photosensitivity.
Commercially available green light lamps designed specifically for migraine use produce wavelengths calibrated to the therapeutic range. Standard green LED bulbs do not produce appropriately narrow-band green light and are not equivalent.
Full guide: Green Light Therapy for Migraine →
Environmental and Lifestyle Modifications
Lighting management at home and work:
- Replace fluorescent overhead lighting with warm-temperature LED or incandescent bulbs (2700–3000K color temperature)
- Use dimmable lighting systems to control intensity
- Install window films or cellular shades to reduce direct sunlight without eliminating all natural light
- Use bias lighting behind computer monitors to reduce screen-to-room contrast
Screen management:
- Enable Night Shift/Night Mode on all devices to reduce blue light output
- Reduce screen brightness to match ambient light level
- Consider specialized migraine-mode screen overlays or software (f.lux, Iris)
- Use matte screen protectors to eliminate specular glare
Trigger identification and avoidance:
- Keep a headache diary (apps like Migraine Buddy, Headache Log) to identify personal light triggers
- Plan outdoor activities with sunglasses and hats for brim-provided shade
- Request accommodations at work (desk away from windows, individual lighting control, ability to use monitor filters)
The Window Tint Medical Exemption: Many migraine patients find that car travel is a significant trigger due to rapidly changing light conditions and glare. In most U.S. states, photophobia patients can qualify for a medical exemption allowing darker-than-legal window tint. This can dramatically improve driving comfort and reduce travel-related migraine triggers.
Full guide: Living with light sensitivity →
Behavioral Approaches
Light desensitization — a structured program involving gradual, controlled exposure to increasing light levels — has theoretical support based on the principle that avoidance worsens sensitization. While controlled clinical trials are limited, some headache specialists recommend graded light exposure programs supervised by a neuropsychologist or vision specialist.
Biofeedback has established evidence for migraine prevention and may indirectly reduce photophobia through its effects on autonomic nervous system regulation and stress response.
Cognitive Behavioral Therapy (CBT) addresses the anxiety, catastrophizing, and avoidance behaviors that commonly accompany chronic photophobia, and has proven efficacy for chronic migraine management.
Related Conditions to Consider
Migraine photophobia does not always occur in isolation. Several related conditions frequently coexist:
Anxiety and light sensitivity — anxiety amplifies photophobia through heightened neural arousal. Treating anxiety often improves light tolerance.
Concussion and light sensitivity — post-concussion syndrome can mimic and exacerbate migraine photophobia, particularly in those with pre-existing migraine history.
Fibromyalgia and light sensitivity — central sensitization in fibromyalgia amplifies photophobia in comorbid migraine patients.
Dry eye and light sensitivity — commonly coexists with migraine and can compound photophobia through a separate peripheral mechanism.
Sound and light sensitivity — phonophobia (sound sensitivity) accompanies photophobia in the vast majority of migraine attacks and shares many of the same central sensitization mechanisms.
When to See a Specialist
Consult a neurologist or certified headache specialist if:
- You have 4 or more migraine days per month — preventive treatment is indicated
- Light sensitivity persists between attacks — interictal photophobia requires dedicated management
- Current medications are not providing adequate relief — many newer options exist
- You want to discuss CGRP inhibitors (erenumab, fremanezumab, galcanezumab, atogepant) which specifically target the migraine pathway
- Botox for chronic migraine is a consideration you want to explore
- Your photophobia is causing significant disability in work or daily life
- You have never received a formal migraine diagnosis — proper diagnosis changes treatment options substantially
Sources
- Noseda R, et al. “A neural mechanism for exacerbation of headache by light.” Nature Neuroscience. 2010;13(2):239-245.
- Burstein R, et al. “Thalamic sensitization transforms localized pain into widespread allodynia.” Annals of Neurology. 2010;68(1):81-91.
- Noseda R, et al. “Migraine photophobia originating in cone-driven retinal pathways.” Brain. 2016;139(7):1971-1986.
- Ibrahim MM, et al. “Green light exposure induces pain relief and decreases inflammatory pain via endogenous opioid release.” Pain. 2021;162(7):1933-1942.
- Digre KB, Brennan KC. “Shedding light on photophobia.” Journal of Neuro-Ophthalmology. 2012;32(1):68-81.
- Wilkins AJ, et al. “Spectral sensitivity of photophobia.” Cephalalgia. 2002;22(7):573-578.
- Katz BJ, Digre KB. “Diagnosis, pathophysiology, and treatment of photophobia.” Survey of Ophthalmology. 2016;61(4):466-477.
- Schwedt TJ. “Chronic migraine.” BMJ. 2014;348:g1416.
- Headache Classification Committee of the International Headache Society. “The International Classification of Headache Disorders, 3rd edition.” Cephalalgia. 2018;38(1):1-211.