Uveitis and Light Sensitivity: Why Photophobia Is a Cardinal Sign
Uveitis causes some of the most intense photophobia in ophthalmology. Learn why uveitis triggers severe light sensitivity, how it's diagnosed, and how it's treated.
For informational purposes only. This site exists to help people with light sensitivity live more comfortably — it does not provide medical advice, diagnoses, or treatment recommendations. Always consult your doctor or a qualified healthcare provider before making any health decisions. Read our full disclaimer →
- Uveitis causes some of the most severe photophobia seen in eye care — the ciliary spasm from iris inflammation creates an intense pain response to any light entering the eye.
- Photophobia, eye redness, and blurred vision are the classic triad of anterior uveitis (iritis) — prompt ophthalmology evaluation within 24–48 hours is essential.
- Cycloplegic drops (dilating the pupil) are a key part of uveitis treatment — they relax the ciliary muscle spasm that drives the pain and photophobia.
- Uveitis has many systemic associations (HLA-B27, ankylosing spondylitis, IBD, sarcoidosis, Lyme) — recurrent uveitis should trigger systemic workup.
- Untreated uveitis can cause permanent vision loss — any new-onset severe photophobia with eye redness should not be managed with sunglasses alone.
Uveitis is one of the most common causes of severe, acute photophobia seen in ophthalmology clinics. The inflammation directly irritates the iris and ciliary body — the structures that control the pupil — creating an intense pain response to any light entering the eye. In many cases, uveitis photophobia is so debilitating that patients wear sunglasses even indoors.
Uveitis affects approximately 1 in 5,000 people annually and is responsible for up to 10–15% of legal blindness in developed countries, making prompt diagnosis and treatment essential.
What Is Uveitis?

Uveitis is inflammation of the uvea, the middle vascular layer of the eye comprising the iris (front), ciliary body (middle), and choroid (back). It is classified by anatomical location:
- Anterior uveitis (iritis) — Inflammation of the iris and ciliary body. The most common form (75% of cases) and the one most strongly associated with photophobia.
- Intermediate uveitis — Inflammation of the vitreous and peripheral retina; less acute, milder photophobia.
- Posterior uveitis (choroiditis) — Inflammation of the choroid; often causes floaters and vision loss rather than photophobia.
- Panuveitis — All layers involved; potentially the most vision-threatening.
Why Uveitis Causes Photophobia
The photophobia of anterior uveitis has a direct mechanical explanation:
Iris sphincter muscle spasm. In a healthy eye, the iris sphincter contracts when light enters, narrowing the pupil. In anterior uveitis, the inflamed iris is hypersensitive — the sphincter muscle goes into painful ciliary spasm with any light stimulus. This is the primary driver of photophobia.
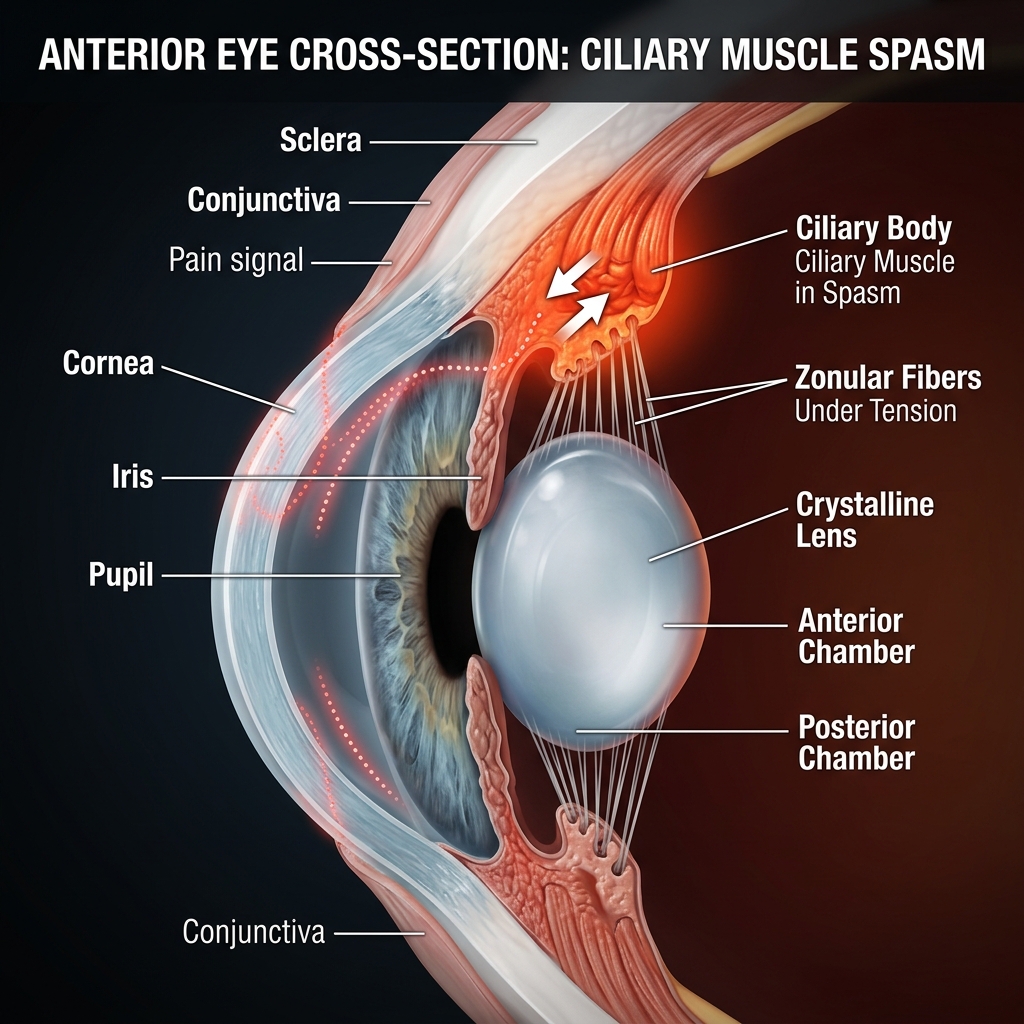
Ciliary muscle spasm. The ciliary body, which controls lens focusing, is similarly inflamed. Spasm of the ciliary muscle causes deep aching eye pain that intensifies with light exposure or attempts to focus.

Inflammatory mediators. Prostaglandins, cytokines, and other inflammatory mediators released during uveitis sensitize the corneal nerve endings, lowering the threshold for pain and light discomfort.
Protein flare. Breakdown of the blood-aqueous barrier floods the anterior chamber with protein-rich fluid, scattering incoming light and amplifying glare.
Causes of Uveitis
Uveitis can be idiopathic (no identifiable cause in ~50% of cases) or associated with:
Autoimmune/systemic diseases:
- Ankylosing spondylitis (HLA-B27 positive) — most common systemic association
- Reactive arthritis (formerly Reiter’s syndrome)
- Inflammatory bowel disease (Crohn’s, ulcerative colitis)
- Sarcoidosis
- Juvenile idiopathic arthritis
- Psoriatic arthritis
Infectious causes:
- Herpes simplex virus (HSV) and herpes zoster
- Toxoplasmosis (most common cause of posterior uveitis)
- Cytomegalovirus (CMV) in immunocompromised patients
- Syphilis, tuberculosis, Lyme disease
Other:
- Trauma (traumatic iritis)
- Post-surgical inflammation
- Certain medications (rifabutin, cidofovir)
Recognizing Uveitis: Symptoms
Anterior uveitis typically presents acutely with:
- Severe photophobia — often described as the dominant symptom
- Eye pain — deep, aching, often worse with bright light or near-vision tasks
- Redness — circumcorneal flush (redness around the iris)
- Blurred vision — from protein flare and inflammatory debris in the anterior chamber
- Small or irregular pupil — sphincter spasm or posterior synechiae (adhesions)
- Tearing
Unlike conjunctivitis (pink eye), uveitis does NOT typically cause discharge, and the redness is concentrated around the iris rather than across the entire conjunctiva.
When Uveitis Is an Emergency
Several forms of uveitis require urgent or emergency evaluation:
- Acute angle-closure glaucoma mimicking uveitis — produces severe pain, photophobia, and halos; requires immediate pressure-lowering treatment
- Endophthalmitis — post-surgical or post-traumatic infection; vision-threatening, requires same-day evaluation
- Herpetic uveitis — requires antiviral therapy within hours to days to prevent corneal scarring
- Behçet’s disease — explosive uveitis that can cause blindness within weeks without aggressive treatment
Any sudden, severe eye pain with photophobia warrants same-day ophthalmology evaluation.
Treatment of Uveitis and Its Photophobia
Topical steroids. Prednisolone acetate 1% eye drops are the cornerstone of anterior uveitis treatment. They suppress inflammation, directly reducing ciliary and iris muscle spasm and thereby relieving photophobia.
Cycloplegic drops. Atropine, cyclopentolate, or homatropine dilate the pupil and paralyze the ciliary muscle, providing immediate pain and photophobia relief by stopping sphincter and ciliary spasm. These drops cause temporary blurred near vision.
Tinted lenses during treatment. FL-41 tinted glasses or wraparound sunglasses significantly reduce photophobia during the acute phase and during cycloplegic treatment (when the pupil is dilated and cannot constrict).
Treating the underlying cause. Infectious uveitis requires targeted antimicrobials. HLA-B27-associated uveitis may require systemic immunosuppression for recurrent disease. Biologics (anti-TNF agents) are increasingly used for chronic recurrent anterior uveitis associated with ankylosing spondylitis.
Monitoring for complications. Posterior synechiae (adhesions between iris and lens), cataract, and secondary glaucoma are the most important complications of recurrent uveitis; regular monitoring preserves vision.
Prognosis
Most isolated anterior uveitis episodes resolve within 6–8 weeks with appropriate treatment. Photophobia typically resolves as inflammation subsides. However:
- Recurrent attacks occur in ~50% of HLA-B27-positive patients
- Chronic uveitis (persistent inflammation >3 months) carries higher risk of vision complications
- Posterior uveitis generally has a more guarded prognosis for vision
Sources
- Jabs DA, Nussenblatt RB, Rosenbaum JT. “Standardization of uveitis nomenclature.” Am J Ophthalmol. 2005;140(3):509-516.
- Rosenbaum JT. “Uveitis: An internist’s view.” Arch Intern Med. 1989;149(5):1173-1176.
- Pato E, et al. “Uveitis: Systematic review.” Clin Exp Rheumatol. 2011;29(5):901-906.
- Digre KB, Brennan KC. “Shedding light on photophobia.” J Neuro-Ophthalmol. 2012;32(1):68-81.